
Universal health coverage (UHC) has been at the forefront of the global health agenda for several years, with renewed enthusiasm following the issuance of the Sustainable Development Goals (SDGs) in 2015. The World Health Organization (WHO) defines UHC as
ensuring that all people have access to needed health services (including prevention, promotion, treatment, rehabilitation, and palliation) of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user [patient] to financial hardship. (WHO, 2010)
Approaches to achieving UHC vary across different applications in different country settings. Evidence is mixed on which approaches are most successful, and unfortunately, not all of them guarantee access to care that is of high, or even adequate, quality. This uncertainty makes decisions about health care reform difficult for countries with limited resources. However, it is clear that without UHC, payment systems are often cobbled together, imposing a burden that many citizens end up bearing through an out-of-pocket (OOP) payment system. Experts agree that most successful systems employ both the public and private sectors, and often use a mix of incentives, structures, and cost containment mechanisms that can be leveraged to assure and improve the quality of care provided. Several global efforts are under way to this end, but if these efforts are not broadened and applied to all settings, including low- and middle-income countries (LMICs), they will be less effective than they could be.
With reference to the committee’s framework in Figure 2-2 in Chapter 2, the discussion in this chapter addresses the “environment” level while highlighting the impacts this level can have on patients, their community, and even individual facilities when incentives are not aligned across levels. The chapter first examines the necessary link between UHC and quality and explains why simply ensuring access and financial protection—although important—is insufficient to achieve effective UHC. It then examines UHC as an opportunity for quality improvement, providing examples of policy levers that can be used within UHC to institutionalize quality in health care systems and reviewing the available evidence on various levers. The third section explores the need for government commitment to achieve quality within UHC, highlighting recent guidance from WHO on creating national quality policies and strategies and presenting illustrative examples of countries that have already undertaken these efforts. The final section presents a summary and recommendations.
THE NECESSARY LINK BETWEEN UNIVERSAL HEALTH COVERAGE AND QUALITY
As highlighted throughout this report, successfully achieving UHC requires financial risk protection and access to high-quality essential health services. Yet, while increasing numbers of people worldwide are being provided with access to health care services, the data and findings presented in Chapter 4 make clear that these services are often not of high quality. For UHC to be effective, the quality of care needs to improve across all key dimensions of quality: safety, efficiency, person-centeredness, timeliness/accessibility, effectiveness, and equity. Quality UHC is achievable with health care services that respond to people’s health needs, taking into account emerging and varied health challenges within each country’s context. To this end, a deliberate focus is required at all points of care—from national to subnational to community units. A 2018 joint report of WHO, the World Bank, and the Organisation for Economic Co-operation and Development (OECD) includes a similar call to action (WHO et al., 2018). After providing a perspective on the suboptimal quality of care in LMICs, the report proposes high-level actions directed at health policy makers, health system leaders, and health care workers. The report argues that these actions would facilitate the achievement of UHC—with “high-quality, people-centered” services. The committee agrees with the argument and recommendations of this joint report, and this chapter seeks to offer additional support for quality as a component of UHC. The sections below explore the interactions and interdependencies within UHC of access, financial protection, and quality—the missing link for ensuring effective UHC.
Expanding Access to Care
As countries are reforming their health care systems, they are giving special attention to incorporating UHC into their objectives. A number of LMICs in Africa, Asia, and Latin America have made substantial progress in their efforts to expand coverage to all population groups. Among the countries that have achieved what can be regarded as UHC systems are Mongolia, the Philippines, Sri Lanka, and Thailand in Asia; Gabon, Gambia, Ghana, and Rwanda in Africa; and Argentina, Chile, Costa Rica, and Cuba in Latin America. Varying levels of health care investment exist in these countries—from $56.66 annually per capita in Rwanda to $29.11 in Costa Rica in 2015 (World Bank, 2018).
Although access is a necessary condition for achieving high-quality care, however, in no way does it guarantee quality. Costa Rica’s massive primary care reform of the 1990s, discussed in Chapter 3, helped reduce child and adult mortality by 13 percent and 4 percent, respectively, for
every 5 years the reform was in place, compared with areas not yet covered (Starfield et al., 2005). Access was certainly part of the country’s strategy, but Costa Rica went beyond access to realize these gains in health outcomes. This is not to minimize the importance of access, however, especially for those patients with complex chronic illnesses. For these patients, access to specialized care can have dramatic effects on their lives. For example, the Vajpayee Arogyashree Scheme (VAS), a social health insurance strategy in India for households below the poverty line, was rolled out in an area with more than 61 million people. Research found that VAS users had lower mortality rates thanks to increased care utilization, better-quality facilities, and earlier diagnosis (Sood and Wagner, 2018).
Reducing the Financial Burdens of Health Care
Since one of the goals of UHC is to reduce the financial hardship associated with health care, it is expected that, regardless of the quality of services in a system, high costs of care are being reduced. A key indicator to consider is the incidence of catastrophic spending.1 Yet, even in the face of the global momentum of and political commitments to UHC, the incidence of catastrophic OOP spending globally has actually increased since 2000 at all household expenditure thresholds (WHO and World Bank, 2017; World Bank, 2016b).
Achieving effective UHC can help reduce this financial burden of health care. In the 1980s and 1990s, OOP payments became a more common method for paying for health care. Yet, of the $500 billion generated by user fees annually worldwide, the World Bank estimates that 40 percent is wasted (The Economist, 2018). A 2009 Rockefeller Foundation report notes that this type of spending is “the most inequitable and inefficient form of financing for health care, leaving patients” without access and further impoverished (Lagomarsino et al., 2009). Moreover, relying on high OOP payments, regardless of income level, violates the spirit of UHC by driving people into poverty and can make the achievement of effective UHC impossible. A high incidence of OOP payments in regions with low domestic funding for health care increases the fragility and instability of health systems and leaves many households vulnerable to financial catastrophe and impoverishment (Okungu, 2015). For millions, the financial burden can cause them to forego needed health care and potentially to become sicker
___________________
1 Catastrophic health expenditure is defined as OOP spending on health care services that consumes a large portion of a household’s available income, such that the household may be pushed into poverty as a result (WHO, 2005). Sustainable Development Goals define two thresholds for catastrophic health expenditures: greater than 10 percent and greater than 25 percent of a household’s available income (WHO and World Bank, 2017).
(Xu et al., 2007). In India, for example, OOP payments account for 70 percent of health care services and are responsible for the impoverishment of 7 percent of the population (Ravi and Sood, 2018). One of the reasons why the VAS example described in the previous section was successful was that it reduced the financial hardship of tertiary care for those in the program, and at a reasonable cost to taxpayers: VAS-eligible households reported 60 percent fewer OOP expenditures for hospitalizations (Sood and Wagner, 2018).
For most people without access to such insurance schemes, high OOP expenses mean that families must provide a large sum of money (relative to their incomes), using multiple avenues, before accessing care. In some parts of the world, requirements for OOP payment deviate so completely from any type of functioning financial system that they lead to detention in the hospital of patients unable to pay, with an appallingly negative impact on the quality of care received. For example, in the Democratic Republic of the Congo (DRC), approximately 54 percent of mothers at one health care facility were detained after failing to pay medical fees for giving birth (Yates et al., 2017). Although they may receive care, these patients are detained for weeks or even months afterward, without continued care, food, or even a bed (Amon, 2015). Box 7-1 describes the example of a detained woman in Uganda. And while many are quick to condemn this practice, as it is certainly a human rights violation and clearly goes against the SDGs and the goals of UHC, the factors contributing to the practice are multifaceted, complex, and not easily resolved without dedicated resources and political leadership.
A cornerstone of UHC should be to end patient detention (Otremba et al., 2015), but doing so is not a simple task. Without a global budget from a national system or mechanisms for insurance and reimbursement, health care facilities naturally rely on user fees to stay open and provide care; otherwise, facilities would go bankrupt themselves, leaving the community without access to care. One option is subsidizing fees based on income level so that OOP payments are not catastrophic for patients and their families, but the health care facility can continue operating. For example, committee members visited hospitals in Goma, DRC, and learned about a community-based health insurance scheme initiated by the Church of Christ in the Congo Baptist Church in 2016. With little investment from the national level, hospital revenues rely on patient user fees to operate. Yet, because the population is very poor, these revenues are often not enough to cover even hospital overhead, such as employee salaries and general infrastructure maintenance. To stay afloat, hospital leaders are hoping to generate more revenue while offsetting the financial risk to patients through this contributory scheme, but doing so will require a concerted and long-term effort. As of December 2017, this effort had resulted in the enrollment of nearly 5,000 members from two districts, with the insurance covering 90 percent of a
standard package of services and patients being responsible for the other 10 percent.2 However, even a 10 percent copayment can be problematic for some families, and without additional funding to subsidize the pool of payments, making this effort sustainable will be an ongoing challenge.
Even when such efforts to make medical care affordable are made, patient detention can still occur. For example, China recently rolled out an ambitious $130 billion package designed to ease the financial burden of health care. Nonetheless, many hospitals still demand payment under threat of detention, reminiscent of corrupt practices described in Chapter 6.
___________________
2 Personal communication, Isaac Muyonga, ComBaptist at the Center of Africa (CBCA), December 15, 2017.
A common practice in China is for hospitals to place newborn babies in holding, preventing new mothers and parents from seeing them until payments are made. With fees totaling up to $19,000, these separations can be prolonged while families try to find the money, which can be especially dangerous with respect to breastfeeding of the babies (Wee, 2018).
Changing this practice of patient detention will require systematic thought, commitment to reform, and mobilization of resources. In Burundi following advocacy against patient detention, for example, user fees for young children and women in labor were eliminated. But with no plan in place to substitute for these lost resources, facilities experienced frequent drug shortages, reduced quality of services, and strain on health care providers (Nimpagaritse and Bertone, 2011). Worse still are the unintended consequences of hospitals refusing to provide care—even emergency care—until a patient can pay. This situation is tragically illustrated by a recent example in Cameroon, where a pregnant woman was turned away at a first hospital that claimed it could not offer the care she needed and then denied service at a second hospital upon arrival with insufficient funds. Following this denial of service, she died on the doorstep of the second hospital while her family member attempted to retrieve her unborn twins from her body (Berlinger, 2016).
Such examples highlight how crucial it is to design the system and financing of health care in a way that ensures quality of care and discourages such deadly practices. While providing care regardless of funding might be considered a step in the right direction, it is not justified if receiving that care sends patients further into poverty and compromises their human rights. Financial support of hospitals is imperative, but many countries will have to grapple with the reality that resources are finite, and thus will need to balance the priorities of funded health care, improved roads, investment in education, and other determinants that may in fact impact population health. These are important trade-offs that countries will need to consider, together with their citizens, clinicians, and other stakeholders, to design the right system. Regardless of the amount of funding directed at health, the focus needs to shift from reliance on OOP payments toward government and private-sector support, in partnership, to achieve UHC. Quality safeguards and assurances need to be incorporated into care offerings. For those populations living in the fragile contexts described in Chapter 5, more global and multipartner solutions will be necessary.
The Insufficiency of Access and Financial Protection to Ensure Quality
As detailed above, while both access to care and protection from financial catastrophe are critically important for keeping people healthy and out
of poverty, they are not enough to truly meet the ambitious goals of UHC. Providing access to care that is of sufficient quality requires a focus on the specific dimensions of quality, as outlined in Chapter 1. The end goals are impacted by what is being monitored and evaluated, and if the number of people accessing care and not encountering financial hardship is all that is being measured, many important elements within the dimensions of quality can be missed, leading to situations in which poor or ineffective care is provided for months or years unnoticed. In 2013, for example, Kenya abolished user fees in public health care facilities in hopes of increasing utilization rates, especially for maternal health care. While this strategy was successful in increasing utilization, which rose significantly for 2 years, maternal and neonatal mortality rates remained unchanged (Gitobu et al., 2018)—this increased access to services did not come with a commensurate increase in human resources, medical supplies, and infrastructure (Otremba et al., 2015). Furthermore, the loss of revenue that results from eliminating user fees, unless replaced by public funding or a mechanism for reimbursement, can lead to worsening quality. All of these issues need to be considered for their quality implications before efforts are made to increase access and utilization (Hercot et al., 2011). This is a key example of the need to link access to quality and to undertake coverage and quality improvement efforts in parallel.
With similar goals of prioritizing access, India created the Rashtriya Swasthya Bima Yojana (RSBY) program in 2008 to provide the rural poor with access to health care. To become empaneled RSBY providers, facilities—whether public or private—must meet certain requirements. Once people have their RSBY card and are enrolled, they can use their card at any empaneled facility, but only for inpatient costs (Upneja, 2015). In practice, however, barriers prevent this from being a successful high-quality program. Empaneled hospitals are located too far from villages to be effective; even if every inpatient hospital close to villages were empaneled, 63 percent of the rural population would still need to travel more than 5 kilometers to access inpatient care (Aitken et al., 2013). The goal of reducing the financial burdens of care for families has been shown to yield mixed benefits as well, with one analysis showing that RSBY provided no significant financial protection for poor households (Karan et al., 2017).
At the same time, however, a perhaps tertiary benefit of this program is that it collects large amounts of claims data with which to conduct evaluation and continual feedback for iterative quality improvement. Currently, the way the data are collected does not automatically make the program a good opportunity for this research, although the potential opportunities certainly exist (Morton et al., 2016). If the right efforts were undertaken using co-design approaches discussed earlier in this report, and if the metrics and indicators used were accurate reflections of quality care and health outcomes, the data collected could offer valuable insight into where resources should be
targeted, and the program could be greatly strengthened. Researchers note that the absence of an accepted quality framework and national benchmarks in India remains a key constraint to adequate data capture and systematic quality measurement (Morton et al., 2016), although the recent introduction of a national patient safety framework suggests that changes may be on the horizon (Indian Ministry of Health and Family Welfare, 2017).
UNIVERSAL HEALTH COVERAGE AS AN OPPORTUNITY FOR QUALITY IMPROVEMENT
The political will and momentum of UHC offer a number of opportunities that can be leveraged to embed quality safeguards within systems and programs. UHC provides new opportunities to make system-wide improvements in health care quality. Moving toward a national health insurance scheme, for example, could help provide access to data on the care-seeking behavior of the population, which could in turn drive health system improvement. New incentives for care coordination and quality improvement could then be created because there would be a baseline understanding of what services were in high demand, where the system was lacking, and where care could be better integrated.
Similarly, the quality of care delivered by the providers and clinics within insurance programs can be monitored and held to high standards through a variety of mechanisms. For example, only hospitals that meet certain quality standards—measured not only by their infrastructure but also by health outcomes—should be available to insurance beneficiaries (Cashin et al., 2018; Mate et al., 2013). Likewise, affiliated doctors should review surgeries performed to ensure that they were warranted and follow evidence-based guidelines as a condition of reimbursement. Rwanda uses this approach to ensure quality within its Community-Based Health Insurance (CBHI) scheme (discussed in detail later in this chapter), which is available to the entire population. Each hospital has an embedded “mutuelle” from the Ministry of Health who reviews all services provided on a regular basis to ensure that they meet quality standards and accord with the essential health care package before reimbursement is issued3 (Republic of Rwanda, 2010). Reimbursement of services using “bundled payments”4
___________________
3 Personal communication, Emmanuel Manirakiza, Gisenyi Hospital, Rwanda, December 14, 2017.
4 Bundled payments are designed to move toward value-based care by predetermining the allowable cost expenditures for an episode of care. This method requires that providers assume some risk, and if the cost of care is higher than the predetermined amount—for example, because of hospital readmission—they will lose that money. However, if they can keep costs lower while maintaining quality standards, they can share in the savings. For more detail, see https://catalyst.nejm.org/what-are-bundled-payments (accessed July 17, 2018).
can also be tied to quality metrics, reducing the incentive to provide more care regardless of whether it is warranted. There are many policy levers for embedding quality. Those that work well for a given region or community will be contextually dependent, and will have to be applied by local leaders and citizens. A variety of these options are discussed below.
Public–Private Partnership
Experts have long debated whether private or public health care is the better answer to the world’s health problems. Some believe that private health care markets will fail because key preventive and public health services often are not valued in a market transaction, and patients’ lack of knowledge and health literacy can leave them vulnerable to overprescription and excessive use of diagnostics (Hanson et al., 2008). Some studies have found private care to be better than public care, while others have found the quality of care in private markets in LMICs to be very low as the result of a poor knowledge base and a lack of effort among doctors (Das et al., 2008). Studies have noted such shortcomings as private providers being less likely to prescribe oral rehydration therapy (ORT) and more likely to prescribe antibiotics (Wagner et al., 2015), newborns being less likely to receive Bacille Calmette-Guerin (BCG) vaccination in a private hospital (Sood and Wagner, 2013), and private patients less likely to be tested for HIV (Sood and Wagner, 2013).
Others have argued that no “public” system is entirely separate from the private sector when it comes to drugs, equipment, and innovation, even to the point of a blended workforce. Das and colleagues (2016) found that doctors who worked in both public and private settings in India (an arrangement that is fairly common in many countries) provided higher-quality care in the private than in the public clinics. On the whole, incentives in the public sector are no better aligned than those in the private sector to provide high-quality care. However, positive associations have been shown between government stewardship and the quality of clinics and hospitals—as demonstrated in Ghana and Kenya, where comprehensive government engagement with health care providers can be influential (Spreng et al., 2014). More research is needed to see which specific engagement strategies are most impactful. While this debate will surely continue, a much stronger evidence base on private-sector engagement is needed to enable better understanding and inform decision making for UHC schemes. It will be difficult for countries to achieve effective UHC without involving the numerous private-sector companies and providers that deliver care.
The committee was curious as to whether a business case can be made for investing in quality that would drive the private sector to improve quality for its own economic benefit. The evidence here is also mixed.
Unfortunately, no peer-reviewed studies have directly evaluated the business case for quality among private providers in LMICs. Analyzing case studies on whether quality improvement costs or saves money, Leatherman and colleagues (2003) found an unclear mix. In most cases, the patient accrued a benefit, and stakeholders benefited from predictable cost savings in the long-term. However, the investor had negligible or uncertain financial returns, making the “business case” ambiguous. This was so in part because patients/consumers were unable to discern quality differences, and in part because quality improvement required using services that were not easily billable to any payer. If benefits to patients and other stakeholders apply at a larger scale, the uncertain “business case” calls for payment reforms and policies that “reward organizations that are willing to invest in quality” (Leatherman et al., 2003). The empirical evidence on this issue is supported by theory that says quality will be underprovided in markets with asymmetric information where sellers know more about quality compared with buyers (Lagomarsino et al., 2009).
Clearly, then, there is a need for systematic investments in improving the quality of care in both the public and private sectors, often in partnership. Both sectors bring strengths and weaknesses, and countries need to bring the two together to work within their own national contexts and address their own priorities to build the right UHC system.
Tapping the Private Sector
Studies have examined very few financing and incentivizing strategies for improving the quality of care provided by the private sector, whether supported by insurance or OOP payments. The authors of a 2017 working paper from the Center for Global Development did study the effectiveness of input and output incentives for private health care providers with different skill levels in India (Mohanan et al., 2017). Focusing on maternity care, the authors found that both input and output incentive contracts resulted in a more than 20 percent reduction in postpartum hemorrhage (PPH). Additionally, they noted that with output incentives, those providers with higher skills were able to achieve large reductions in PPH, but those with lower-level skills and training failed to do so. The rate for both groups was the same with input incentives, showing that pay-for-performance schemes could focus on input incentives regardless of skill levels.
Another key financing component that can improve the quality of services is strategic purchasing (Cashin et al., 2018). Strategic purchasing, as opposed to passive purchasing, makes use of information on performance and a payment mechanism that incentivizes certain behaviors and results, such as improvements in health system performance, improved efficiency in resource use, and improved quality (Cashin et al., 2018). Strategic purchas-
ing involves decisions on what services to buy, what service providers to choose, and how and how much to pay providers (Figueras et al., 2005). These decisions would be optimally supported by such mechanisms as monitoring the performance of providers and knowing the different institutions that have purchasing functions. Goldfarb and colleagues (2003) identify six key means by which purchasing ensures quality of services:
- collecting accurate information on provider or health plan performance;
- contracting with providers that meet the quality threshold as defined;
- partnering with providers or health plans to improve quality;
- promoting “Six-Sigma” quality, an industry-based model for minimizing errors and waste;
- enhancing consumer awareness and understanding of quality services; and
- using incentives to reward or punish providers of poor-quality services.
The committee encountered several anecdotal examples of successful high-quality care delivery by private providers that could be replicated. For example, PurpleSource in Nigeria, a private integrated health care provider, set its own goal of improving access to quality primary health care services. It used partnerships to minimize the risk of counterfeit medications and used accreditation within its clinic network for quality assurance. With a deep customer development focus and using a hybrid strategy of improving efficiencies, leveraging economies of scale, centralizing management, and lowering costs without compromising quality, it applied lean execution methods with multiple pivots until it started seeing results (Sunmonu, 2017) (see also Box 2-2 in Chapter 2).
In another example, Narayana Health in India has been able to deliver high-quality services at affordable cost through such process innovations as configuring assets in a hub-and-spoke model facilitated by telemedicine and increasing the quantity of services provided (Govindarajan and Ramamurti, 2013). Narayana Health performs more open heart surgeries than anywhere else in the world, also increasing physician productivity; surgeons at Narayana perform 400–600 procedures per year, compared with 100–200 in the United States (Taylor et al., 2017). Similarly, providers in another system in India, Aravind Eye Care, perform high numbers of eye surgeries (McKinsey’s Health Systems and Services Practice, 2011). This high volume of procedures makes it possible to develop and continually update protocols for patients of varying risk levels, enabling specific and evidence-based care for every type of patient. Both of these hospitals have also used task shifting to maximize efficiency and ensure that all providers
perform only “tasks they are uniquely qualified to do” (i.e., working at the “top of their scope of practice”) (McKinsey’s Health Systems and Services Practice, 2011; Taylor et al., 2017).
Policy and Financial Levers to Institutionalize Quality
A variety of mechanisms, especially for mixed health system stewardship, can be used to incentivize meeting quality-of-care goals among multiple players in the system (see Figure 7-1). These mechanisms have produced good outcomes in a variety of high- and middle-income countries, but have yet to be adopted in low-income countries. Pooled financing models influence health care quality in the private sector in many ways, but when they are paired with strategic purchasing, an insurer can develop a “network of preferred providers for insured patients to choose from” (Lagomarsino et al., 2009, p. 22). Through this model, insurers can assure quality by providing clinical protocols and training to approved providers and mandating that they meet basic quality standards (Lagomarsino et al., 2009). This approach can be taken a step further through pay-for-performance models that use financial incentives to foster additional quality improvements (Gottret and Schieber, 2006). If the levels of quality are not maintained by a provider, the insurer can remove that provider from the network or take other actions, such as withholding payments.
In addition, these types of active, or strategic, purchasing measures can enable cost containment, align services with population needs, and balance provider payment. Thailand’s UHC scheme, for example, practices active purchasing to control costs while also being responsible for achieving impressive health outcomes (Okungu, 2015). In fact, government health expenditures in Thailand total only 3 percent of its gross domestic product (GDP) (Limwattananon et al., 2013), and the country has met the WHO recommended threshold of less than 20 percent of total health expenditures as OOP spending (Xu et al., 2010).
To identify the best options for policy and financial levers and their available evidence, the committee conducted a rapid review of current research on strategies for health care improvement being tested in countries (see Appendix B for the review protocol). More than 100 studies were analyzed for their impacts on health outcomes. The committee found that the evidence is mixed across many interventions and several countries and continents. Thus, there is clearly a need for additional research on potential interventions to show how they can be implemented sustainably at scale. (Note that the examples from various countries presented in boxes throughout this section are intended to provide additional context, but they were not included in the rapid review and should be considered separate examples of these types of incentives.)
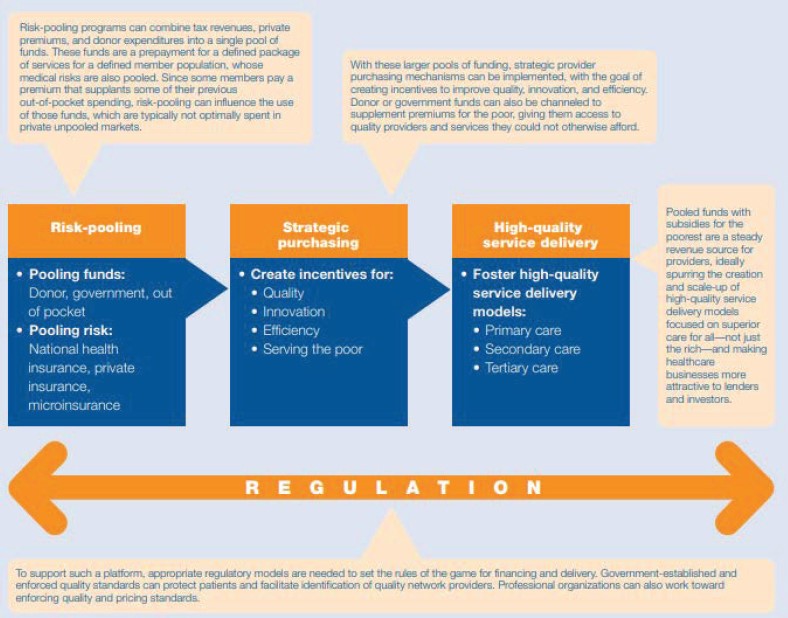
SOURCE: Lagomarsino, G., S. Nachuk, and S. S. Kundra. 2009. Reprinted from Public stewardship of private providers in mixed health systems: Synthesis report from The Rockefeller Foundation-sponsored initiative on the role of the private sector in health systems in developing countries. (p. 4), by Lagomarsino, G. S. Nachuk, and S. S. Kundra, 2009, Washington, DC: The Rockefeller Foundation. https://www.r4d.org/wp-content/uploads/Public-Stewardship-of-Private-Providers-in-Mixed-Health-Systems.pdf (accessed June 4, 2018).
Public Reporting and Community Engagement
Several studies investigated the role of public reporting and community engagement in improving patient safety and reducing risk presented by health workers (Alhassan et al., 2015; Liu et al., 2015, 2016; Tang et al., 2016; Yang et al., 2014; Zhang et al., 2014). The literature reviewed on public reporting does not lend strong evidence to support its effectiveness in reducing overprescription of antimicrobials. Overall, the evidence is highly mixed, and the only study with consistent findings found that public reporting decreased prescriptions for gastritis but increased those for hypertension. Moreover, most of the studies had a methodological weakness in that they analyzed the effects of the intervention too soon after its introduction. Liu and colleagues (2015) found a lag in the effect of public reporting on prescribing practices. Thus, the findings are uncertain in that the effects of this intervention could be undermeasured, and the sustainability of the reductions in prescribing patterns is unknown.
Alhassan and colleagues (2015) found that community engagement did appear to improve accountability and leadership, but did not have a significant impact on quality of care. The varied impact of the gender composition and type of community group on the particular risk area scores warrants further research.
Additional research is needed on public reporting, examining, for example, its sustainability and its effect on prescription practices depending on patient or provider characteristics. Additional research also is needed on community engagement, such as how the composition of community groups can influence its impact. In addition, research on the unintended consequences of both of these strategies is needed.
Mobile Health (mHealth)
mHealth is among the multiple digital health technologies and tools highlighted in Chapter 3. Because mobile phones were available across many types of settings long before broadband 3G access or smartphones, a fair amount of research has been conducted on mHealth interventions with respect to health outcomes. However, complaints often arise about too many pilots or interventions or target groups being too narrowly focused, making it difficult to generalize findings.
The committee identified two systematic reviews on mHealth interventions (Kallander et al., 2013; Stephani et al., 2016), but the small number of studies included and the settings where these interventions were implemented make it difficult to apply and generalize the findings or recommendations. The reviews did find that mHealth interventions can be effective, and can improve the accuracy of health workers’ data submission and clini-
cal decision-making skills and have positive effects on noncommunicable diseases (NCDs) (Kallander et al., 2013; Stephani et al., 2016). However, the authors also caution that these interventions can cause workers to focus too much on technology and less on the patient, potentially diminishing person-centered care. Kallander and colleagues (2013) note that few evaluations of mHealth have addressed low-income countries, and that sustainability and scalability are a challenge.
Clinical Decision Support (CDS)
CDS, which often has a technology component, has been examined as a possible intervention for quality (Ali et al., 2011; Anchala et al., 2015; Duysburgh et al., 2016; Maia et al., 2016; Mensah et al., 2015). However, many of the studies reviewed measured the impact of time spent on care or workflow, rather than the impact on health outcomes. These studies did identify positive effects on nonhealth outcomes, finding that CDS is feasible to implement, is accepted by providers, improves workflow, and is cost-effective (Anchala et al., 2015; Duysburgh et al., 2016; Maia et al., 2016; Mensah et al., 2015). Of the three studies that measured outcomes, only one found that CDS had a positive impact (Anchala et al., 2015). Although the studies identified lend weak evidence for CDS as a tool for quality improvement, they do indicate that it can improve process efficiency and cost-effectiveness. Should additional evidence on the impact of CDS on health outcomes be developed, customization and implementation of this strategy in LMICs could make it possible to leapfrog infrastructural deficits that occur in high-income countries.
Workforce Training
The committee reviewed multiple studies on workforce training (Bassuni and Bayoumi, 2015; Bazant et al., 2014; Bergh et al., 2015; Vasan et al., 2017). Although Bassuni and Boyoumi (2015) and Bazant and colleagues (2014) did not analyze health outcomes, their analysis of provider perception lends vital insight applicable to health care quality. Specifically, they highlight that providers’ knowledge of care processes and the occurrence of adverse events can lead them to improve their own behavior (Bassuni and Bayoumi, 2015; Bazant et al., 2014). Vasan and colleagues (2017) report the important finding that little is known about the elements of performance improvement and training for primary care workers. Bergh and colleagues (2015), on the other hand, provide strong evidence for the introduction of emergency obstetric and neonatal training. As more countries invest in community health workers, filling this knowledge gap will be important. Bassuni and Bayoumi (2015) and Bazant
and colleagues (2014) also provide valuable insight on the creation of a quality and safety culture through the eyes of providers, demonstrating that increasing skills through training and supported supervision can improve perceptions of a work environment and thus the reception of constructive feedback. This strategy can also be implemented through nurse mentorship programs to decentralize the management of disease.
These findings, however, need to be supplemented by future research on health outcomes and insights from patients. Likewise, the findings of Vasan and colleagues (2017) call for future research on comparative intervention trials and the establishment of clear global standards for professional performance initiatives. Lastly, although Bergh and colleagues (2015) did find positive results for the obstetric and neonatal training program they studied, it was adapted from a high-income setting and may not be easily transferred. Future studies are needed to investigate the contextual and socioeconomic conditions in LMICs in order to improve the adaptation of the training program.
Accreditation
Accreditation is a common mechanism for improving the quality of facilities, both within and outside the health sector around the world. The committee considered several studies, including a systematic review examining accreditation as an intervention for quality, in this review (Al Tehewy et al., 2009; Devkaran and O’Farrell, 2015; Halasa et al., 2015; Ng et al., 2013; Peabody et al., 2008; Saut et al., 2017). Collectively, the studies reviewed investigated the impact of accreditation on quality improvement, organizational and financial factors, process and health outcomes, hospital quality activities and measures, level of quality, and patient and provider satisfaction.
Saut and colleagues (2017) found that accreditation status in Brazil was significantly associated with patient safety and quality management activities. Similarly, Halasa and colleagues (2015) found that accredited hospitals compared with nonaccredited hospitals in Jordan had decreased rates of readmission to the intensive care unit (ICU) in 24 hours, reduced staff turnover, and improved completeness of medical records. Peabody and colleagues (2008), using clinical vignettes to calculate quality scores, found that accredited providers and institutions in the Philippines scored higher than nonaccredited facilities. Lastly, Al Tehewy and colleagues (2009) found that accredited health centers in Egypt had higher patient and provider satisfaction and performed better on patients’ rights, information systems, compliance with care standards, and recording of patient visits in records. Although not included in this review, two nationwide accreditation programs, in Turkey and Jordan, are described in Box 7-2.
These positive results, however, need to be qualified. Although Saut and colleagues (2017) found positive associations with accreditation, they did not find a correlation between accreditation and monitoring of safety goals, nor did they measure outcomes. Ng and colleagues (2013) found clinical impacts that included improved patient safety, reduced medical errors, and increased public reporting. However, some findings contradicted these results, which were not deemed to provide strong evidence for the use of accreditation. Devkaran and O’Farrell (2015) found perhaps the most mixed results. They analyzed the impact of accreditation on a set of quality measures that included patient assessment, laboratory safety, surgical procedures, medical errors, anesthesia and sedation use, use of and access to patient records, infection control, reporting of mortality and morbidity, and safety goals. While they found a significant improvement in quality leading up to accreditation, 26 percent of the measures had reduced scores postaccreditation, with only 2 percent showing improvement.
Ng and colleagues (2013) also report on a variety of factors that can affect the impact of accreditation on quality improvement. Teamwork culture, for example, is important for the willingness of staff to undertake improvement efforts, and if supplemented by leadership, can increase the likelihood that accreditation will advance quality improvement.
Overall, the studies reviewed provide a growing base of evidence that accreditation can create a safety and quality culture in addition to yielding real improvements in health outcomes. However, the study results are mixed. Peabody and colleagues (2008) attempted to investigate these mixed results, but their study’s small sample size made it difficult to do so. Overall, the results do not support accreditation as a tool for quality improvement in all settings, nor do they support its use for quality improvement in isolation. The latter point is crucial. Although not always the case, third-party payers may contract exclusively with accredited institutions. Yet, the influence of accreditation standards is not fully explored in the literature. There is a chance that meeting these standards is merely done as a formality and not as a result of a quality improvement culture. Additional research is needed on how accreditation can create a quality improvement culture, on the linkage between accreditation and clinical indicators, on compliance with the standards, and on innovative ways to track improvements (beyond standards set by accreditation requirements).
Pay for Performance (P4P)
Whether the various financing strategies in use in health systems around the world have significant impacts on quality remains uncertain. Among these, P4P has been the subject of extensive research using a mix of methods and has been analyzed across several systematic reviews (Eichler et al.,
2013; Suthar et al., 2017; Witter et al., 2012). While P4P has been shown to improve utilization of services, quality of care, and patient outcomes, the strength of the evidence is weak, and more studies with strong research designs are needed to understand the impact of P4P on quality of care. Furthermore, given that P4P is not a uniform strategy and can involve making several design choices, more studies are needed to document the implementation of P4P programs. Lastly, more studies are needed to understand the potential unintended consequences of P4P schemes. Box 7-3 describes examples of P4P schemes in different countries and their effects on quality (although these studies were not included in the committee’s rapid review).
Other Mechanisms for Financing Health Care
The starting point for health care financing is understanding what is possible and what level and mix of funding are available, what the channels are for health care expenditures, and how sustainable they will be over time (Xu et al., 2018). The main sources of revenue for health care systems are currently tax revenue, mandatory social health insurance contributions, voluntary private insurance, or a mixed system (World Bank, 2016a). Public sources can include government revenue, social security contributions, and even external resources from international donor countries and organizations. However, some countries, even those of low-income status, elect to provide national health insurance instead of directly providing care, and can build in methods for ensuring that the insurance is used only where services meet quality standards. An example of a national health insurance fund is Rwanda’s CBHI program, referred to previously with respect to its use of the “mutuelle,” which is based on a partnership between the national and local governments (through their districts) and the community (see Box 7-4).
A Framework for Improvement in Health Care Quality
Clearly the path to effective UHC is not straightforward, and every country encounters challenges along the way, especially in covering its poorer populations, who often work in the informal sector and thus lack access to typical employer insurance. The committee understands that the pursuit of UHC is a difficult and multifaceted process, but again strongly emphasizes the need to include and evaluate quality along with the important issues of access, coverage, and financial protection. Much of the research conducted throughout various health systems is focused on the results of efforts addressing access, equity, and utilization rates. Very few studies have looked at health outcomes, patient or family well-being, or other quality indicators, making it difficult to understand which approaches
result in higher-quality care and better health for populations, versus cost savings or improved efficiency.
Regardless, knowing that most countries will have a mix of insurance, government, and private-sector roles in health care, a framework is needed to understand how quality, coverage, and financial protection can be considered and accounted for as systems reform. Mate and colleagues (2013) developed a framework for improvement in health care quality that considers how insurers interact with other stakeholders to promote a cohesive national strategy within a country (see Figure 7-2). This framework can serve as a guide to policy makers as they think about quality improvement in the context of UHC. Depending on the country and employment demographics, the disease burdens, and the political leadership, the mix of options in the “ideas” and “execution” circles of Figure 7-2 will differ. But regardless, the stakeholders that need to contribute “will” to improvement efforts are likely the same, and within the same context of working to improve the quality of health care for their populations. Yet, political will for improving quality may occur slowly without adequate advocacy and public demand. The following are some of the questions policy makers need to ask in seeking to advance improvement:
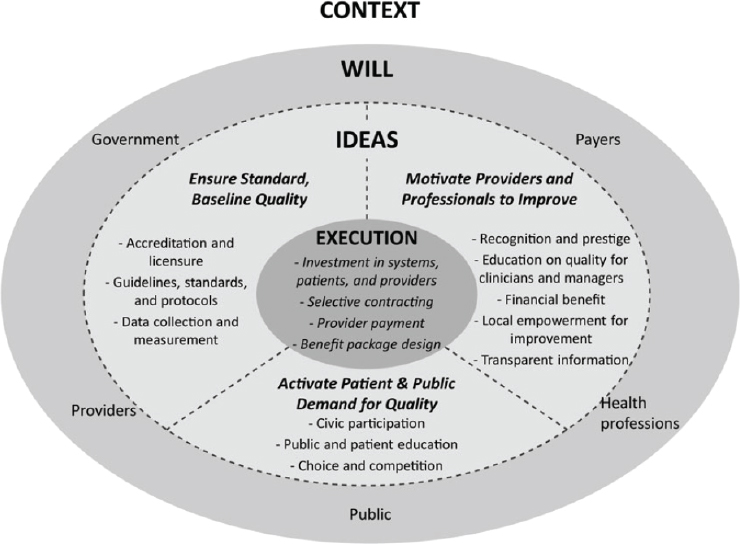
SOURCE: Mate et al., 2013.
-
Do we have leadership and will to improve health care quality?
- Is improving health care quality a national priority?
- What are we doing to motivate and equip health care professionals to improve quality?
- Do providers have the technical skills to provide high-quality care?
- Do providers have the right incentives? Are higher-quality providers rewarded in terms of prestige, reputation, or financial benefit?
- Are providers working in learning health care organizations that have a mission to improve quality of care and empower providers to do so?
- Do providers have access to decision support tools based on evidence-based guidelines?
- What are we doing to activate patient demand for quality?
- Do patients have adequate health literacy?
- Do patients understand what level of care is to be expected?
- Do patients understand the consequences of poor-quality care?
- Do they have the tools and resources to distinguish between high-quality and poor-quality providers?
- Do they have the ability to choose high-quality rather than low-quality providers?
- Is high-quality care affordable?
- Are payers focused on improving quality?
- Does insurance cover high-quality care?
- Are we using selective contracting and provider payment to improve quality?
- Are payers monitoring quality and reducing the use of inappropriate or poor-quality care?
- Do we have a regulatory or legal framework for ensuring access to high-quality care?
- Do we have a robust system for licensing and accreditation of providers?
- Do we have a system for reducing counterfeit or substandard products?
- Do we have the leadership and organizational structure to provide quality health care?
- Do different parts of the system coordinate care?
- Is there accountability?
THE NEED FOR GOVERNMENT COMMITMENT TO QUALITY WITHIN UNIVERSAL HEALTH COVERAGE
Taking on the challenge of UHC requires a deep commitment from a country’s leaders to serving all of its people. Among those countries that have seen successes, an overarching characteristic is strong political leadership for stewarding coverage expansion policies. In Ghana, Sri Lanka, and Thailand, for example, a populist political process (established initially for election purposes) created the momentum for free health care at the point of service (Agyepong and Adjei, 2008; Gunatilleke, 2009; Missoni, 2010). Other important examples include Sri Lanka’s social welfare program (Gunatilleke, 2009) and Thailand’s health system development, which includes maintenance of institutional knowledge via retention of key personnel (Missoni, 2010; Tangcharoensathien et al., 2010).
Systems that are in such dire straits that patients—most often women and their newborn babies—are being detained for payment need multifaceted and immediate interventions. The Chatham House report (Yates et al., 2017) emphasizes the need for policy interventions that can deliver immediate impact, such as banning the practice of patient detention completely with enforcement to follow, as well as compulsory public financing mechanisms to steer countries away from direct-charge mechanisms that contribute to hospitals serving as debt prisons and toward prepayment. As countries transition from severely underfinanced health systems to those that have sustainable and equitable funding sources, leaders will be key in ensuring that UHC policies help improve quality.
Leadership and Stewardship
Leadership for quality can manifest in different ways. In the case of Nigeria, the success of the National Quality Strategy (NQS) is attributable to the involvement of the leadership of the Federal Ministry of Health (FMOH) and its broad group of stakeholders in the strategy’s implementation (Wickham et al., in press). Stakeholders represented regulatory agencies, implementing partners, the private sector, and patient groups. The many different workshops, meetings, interviews, and activities undertaken by the FMOH and nongovernmental organization (NGO) partners helped increase the demand for high-quality care. Stakeholders who were engaged from the beginning are now starting to carry out their own quality-of-care initiatives in line with the country’s overall strategy, ranging from accreditation regulations, to patient empowerment through information access, to compulsory data reporting (Wickham et al., in press). Stakeholders reported a clear commitment at the state level and increases in demand, openness, and trust—all likely contributing to the success of the NQS implementa-
tion. However, it was national-level leadership and commitment from the Minister of State for Health that drove the success.
On a broader scale, in addition to commitment from leadership and a clear vision for improvement, country experiences have shown that structures at the national, regional, and hospital levels are needed to coordinate and lead the implementation of activities related to a national strategy (Wickham et al., in press). During Ethiopia’s journey toward an NQS, for example, the federal government established a new Health Service Quality Directorate. A Steering Committee for National Quality was also created to convene multiple stakeholders and agencies on a regular basis to review progress in implementing the NQS. Furthermore, the country is developing a Quality Technical Working Group to bring together a broader set of partners supporting quality-related work. This example is being duplicated at the subnational level, with quality units being formed within regions; focal persons being assigned to coordinate implementation at the zonal level; and hospitals and health centers, respectively, being expected to have quality units and committees (Wickham et al., in press). Further supporting these newly established structures will be well-trained experts in quality who are able to operationalize the strategy and continue to iterate in a continual improvement process. This expertise, if not found in house, can be sought through linkages with academia and other health partners. Government structures and dedicated personnel, however, will have limited effectiveness if there is high administrative turnover or loss of institutional memory.
Beyond commitment and the establishment and maintenance of government structures, the success of UHC designs and payment systems will depend on the political acceptability and sustainability of the financing system. In fact, it has been found that UHC is less likely in societies with low social solidarity (e.g., political or economic divisions) (Stuckler et al., 2010). The institutional universalism described by Okungu and colleagues (2018) as making a noncontributory financing approach successful requires a high level of collective responsibility among the population, which in some countries, regardless of income level, is difficult to imagine.
National Quality Policy and Strategy Development
With so many countries at various stages of quality control and improvement and a clear need for many systems to deliver better care, WHO recently developed a handbook with country-level input to support those countries interested in improving their health care systems (WHO, 2018a). While improvement is traditionally viewed as a linear process, the handbook makes an argument for moving toward a more triangular or circular process whereby “implementation experience drives policy and strategy development [and] can build a sense of ownership among those implementing
to ensure products are grounded in realities” (WHO, 2018a, p. 11). This argument aligns with the committee’s call for systems thinking, integrated co-design, and meaningful engagement with stakeholders in evaluating and improving any health care process, as outlined in the design principles presented in Chapter 2 of this report. Ongoing relationship building and engagement with the entire health care team, including patients and families and blending top-down and bottom-up approaches, are needed to ensure that interventions tested in the real world are being incorporated into policies and strategies.
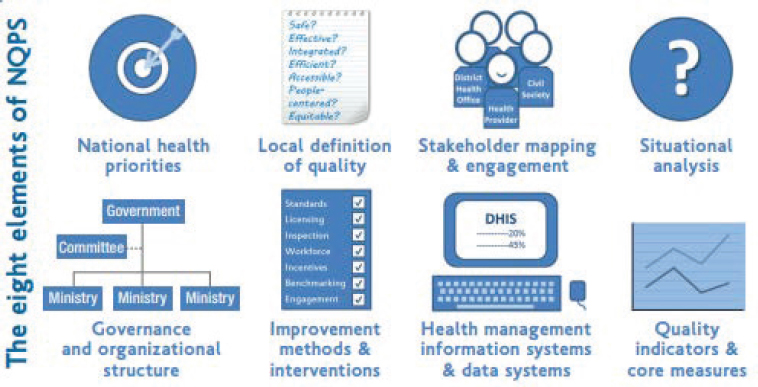
The WHO team reviewed more than 20 existing quality strategies across LMIC settings in developing the handbook, which is intended to guide countries in the development and implementation of their National Quality Policy and Strategy (NQPS). The process is organized into three stages: policy development, strategy development, and tools and resources. Eight key elements are identified as requirements in the policy and strategy development stages: (1) national health priorities, (2) local definition of quality, (3) stakeholder mapping and engagement, (4) situational analysis, (5) governance and organizational structure, (6) improvement methods and interventions, (7) health management information systems and data systems, and (8) quality indicators and core measures (see Figure 7-3). This committee endorses that list.
Because the handbook is intended for use by authorities, stakeholders, and external partners involved in the development of an NQPS, the guidelines account for the fact that countries are in different stages in the development and implementation of national initiatives. The handbook provides guidance on how to develop a national quality policy, either as a stand-alone document or incorporated into the overall national health policy.
The policy development stage of the process aims to acknowledge the existing systems and factors that will contribute to the national quality policy. The handbook states that the national policy should be based on agreed ambitions that should intentionally become the agreed course of action (WHO, 2018a). The strategy development stage entails the process by which the policy is enacted. It should include a time frame for the various activities to be launched and consider and plan for the various practical concerns that may arise when translating the policy into action. The same eight elements included in the policy development stage should also be applied in this stage, and even simultaneously when appropriate. WHO acknowledges that advocacy efforts may be required to incorporate goals and priorities related to quality successfully across the health care system and ensure that they are present in national health planning and budgeting in addition to the NQPS. This, again, will require commitment and political will from the highest levels of leadership—whether at the level of a health
NOTE: NQPS = National Quality Policy and Strategy.
SOURCE: WHO, 2018b.
care facility, care delivery network, or national government entity (WHO, 2018a). The “Tools and Resources” section of the handbook describes how to access and select the tools needed to implement and sustain successful NQPS strategies.
A strength of the WHO handbook is the adaptability of strategies to countries regardless of their stage in the design and implementation of an NQPS (WHO, 2018a). For example, Ghana developed an NQPS for 2017–2021 through a collaborative approach, led by a steering committee, managed by a Ministry of Health team, and evaluated by patients and providers (Ghana Ministry of Health, 2016). This collaborative effort is intended to encompass the entire health care system, categorized by country priorities: maternal health, child health, malaria, epidemic-prone diseases, NCDs, mental health, and geriatric care. Included are measures of improvement in health outcomes, strengthening of systems, and patient-centeredness. The guiding principle of the strategy is to improve health care coordination, so it incorporates the public and private health care sectors, emphasizes partnership with patients and providers, and establishes feedback loops to guide quality improvement at all levels (Ghana Ministry of Health, 2016).
Not every country’s policy and strategy will be the same. Depending on the emphasis placed on certain areas—based on national priorities—plans will manifest differently to address certain gaps. The selection of goals may also be related to recent outbreaks or events that are fresh in a country’s collective mind. For example, Ethiopia’s ultimate aim is to “consistently ensure and improve the outcomes of clinical care, patient safety,
and patient-centredness, while increasing access and equity for all segments of the Ethiopian population, by 2020” (WHO, 2018a, p. 35). Namibia’s strategy, on the other hand, is aimed instead at providing a framework for the implementation of quality management initiatives at all levels using four key objectives as a guide: (1) improve quality management systems and accountability, (2) ensure client-centered care and empowerment of consumers, (3) improve patient and health worker safety, and (4) improve clinical practice (WHO, 2018a). Different still, is the strategy of Sudan, where quality is defined as “providing the best possible patient-centred care using available resources and evidence-based practice” (WHO, 2018a, p. 36).
Accountability
These processes of quality improvement are thoughtful methods of care management. During his testimony to the committee in Nairobi, Maina Boucar, from University Research Company’s Regional Office for Francophone Africa, highlighted several instances of low-resource countries implementing quality improvement efforts with corresponding success. He noted that tangible improvement is possible where leadership is strong, but that these types of interventions cannot be seen as an external effort, and need to be owned by and implemented within organizations. He stressed that accountability for this improvement and assurance of quality is crucial. One of his final reflections was on how to gain buy-in from local leaders and managers, as well as solicit the voices of consumers, to achieve the long-term sustainability of these quality efforts, which otherwise would certainly be in question.
The authors of a 2009 report on public stewardship of private providers in mixed systems also support the notion of accountability, and highlight the importance of “educating and incentivizing patients to demand the most beneficial services,” increasing the “supply of high-quality services,” and reducing “inappropriate provider behavior” (Lagomarsino et al., 2009, p. 6). Examples of such educating and incentivizing interventions include social marketing; conditional cash transfer; rural cooperatives; and trusted sources of knowledge within the community, such as consumer associations or citizen complaint lines. At the core of these efforts, however, is the aim to build health literacy.
Building Health Literacy
Health literacy, or “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (IOM, 2004, p. 4), is vital to building public demand for quality. While individuals with low health
literacy can understand what poor-quality care looks like, they may not be able to articulate what level of quality is expected. Beyond such vital aspects as good communication and respect, other indicators of high-quality care may be unknown to the general population. For example, people in many countries can often associate such things as cleanliness or wait times with quality instead of evidence-based care or correctly prescribed antibiotics. Other indicators of quality may include providers knowing that ORT is needed for diarrhea or when it is necessary to provide intravenous fluid. Of course, the attainment of full health literacy on all treatments is unrealistic. However, an understanding of what services should be delivered and what providers should be present and available is not. While achieving this level of health literacy may require robust community outreach and education efforts, it will offer some balance to the asymmetry that exists around the world between the patient and the physician. In most places, when people seek care from a health care facility, they are reliant on the provider for all knowledge about their condition, and they are unable to actively choose to avoid underperforming providers (Miller and Babiarz, 2013).
Absent an ability to articulate what is expected during a visit, or in response to certain illnesses, a population will have diminished bargaining power and may mistakenly continue using facilities of poor quality. A similar line of logic was used by researchers at the Massachusetts Institute of Technology to address an equity issue in a rice distribution program in Indonesia. Although the program targeted the poorest in the country, in reality only 50 percent of its volume was reaching those individuals. Through the phased introduction of an eligibility postcard, which informed individuals what they were entitled to, beneficiaries were able to demand their full ration. In fact, following this intervention, it was found that experimental village beneficiaries had received 26 percent more rice than those in control villages (Beaubien, 2018). In line with the committee’s suggested principles of co-design and empowered users at the center of the health care system, building the health literacy levels of populations will be a critical factor in raising levels of quality in all settings.
Generating Public Demand
Neither public- nor private-sector leaders will likely change of their own accord, as is fundamentally called for in this report, without a corresponding demand for better care from their populations. Accordingly, it will be necessary to generate stronger demand for high quality, educate patient populations in health literacy, and create incentives for change that will be attractive to all parties. It is important to note that for a significant portion of this work, the onus is on patients or users of the system to increase their health literacy, even though they are the ones falling through cracks within
a complex system of policies and institutions (Hudson and Rikard, 2018). Nonetheless, as with other market-driven solutions, the responsibility for improvement should fall on companies and providers. A review of strategies for preventing stillbirth found that demand creation at the community level was a successful strategy for improving uptake of services, but it was most effective when coupled with supply-side efforts to improve quality of care and system strength (Bhutta et al., 2009).
Embracing the technological advances and shifts to consumer ownership of health data and health care decision making described in Chapter 3 will require that the health care industry transform its business models to incentivize providers to enhance the care experience, reduce waste, and improve quality (Hudson and Rikard, 2018). For example, Chinese consumers are some of the most digitized in the world, and spend more than one-fourth of their online time on medical-related matters (Guo, 2017). As they have become more perceptive in exploring their conditions, their treatments, and even their physicians’ professional work, they have been driving the demand leading to a more joint decision-making model between physicians and patients. In some cities, a survey found that 47 percent of patients requested a prescription change, with 42 percent of their physicians approving the change (Guo, 2017). This trend will likely spread to other countries as they increase their connectivity and digital familiarity, but ensuring that patients possess high levels of health literacy to inform their shared decision making will be crucial to ensuring that high-quality care is provided.
Use of Coverage to Develop Learning Health Systems
Aside from OOP payment schemes, the majority of health systems are backed by some type of insurance coverage or government or donor investment. Health system leaders need to think about how this funding for health care facilities and providers, often as reimbursements for services, can be leveraged for improved quality. As discussed in this chapter, there are contractual and other mechanisms that can be used to build quality assurance and improvement into coverage systems, but they need to be supported by strong political commitment and leadership, as well as accurate metrics and measurement to demonstrate effects on quality and health outcomes. To be most effective, these metrics should be tracked over time, not just at a single point in time, to show rates of improvement. Those measuring and tracking also need to be sensitive to how the results are being used, ensuring that they are being used to drive continual improvement, incentives, and feedback, not for punishment and reprisal.
Using the previous example of PurpleSource in Nigeria, its leaders realized that achieving their goal of access to high-quality primary care
services for mostly poor and informal workers in their network would be a long-term effort. As part of that process, they employed the principles of co-design and human-centered design discussed in Chapters 2 and 3 to include their employees in the design and implementation of any new experiments or changes in care delivery. They also spent time learning about their patients and where bottlenecks existed in the patient journey and the health care delivery process that were costing money and leading to poorer health outcomes. From these efforts, they were able to define a small set of traction metrics and focus on the right product–market fit for primary care in their densely urban context. As they learned, they incorporated those lessons back into their model and pivoted where necessary to continue to improve. The result has been up to 80 percent of primary care hospital visits costing 40 percent less and taking less than one-fourth of the time (Sunmonu, 2017).
Similarly, Thailand’s experience attests to the potential impact of continual research, monitoring, and updating of a universal coverage program (Missoni, 2010). Chapter 8 explores this concept of a learning health care system in greater detail, with specific examples of how it can be operationalized in various contexts.
SUMMARY AND RECOMMENDATIONS
Political will and committed executive and operational leadership are essential to financing and suitably equipping the health sector to deliver effective UHC. However, the methods and pathways for pursuing this goal are numerous, and will require contextual application and engagement and co-design with citizens to develop the best system for each country. India saw success with its VAS social health insurance program, in which patients experienced lower mortality rates thanks to increased care utilization, better quality facilities, and earlier diagnosis, as well as 60 percent fewer OOP expenditures for hospitalizations. Costa Rica undertook massive primary care reform, helping to reduce child mortality by 13 percent for every 5 years the program was in place. Even more countries are now starting on their journey to improve the quality of their health care. Global resources and learning networks exist, providing technical and policy guidance on how to establish NQPSs, as well as lessons learned from other countries that are working toward these goals.
Regardless of the options chosen, a focus solely on access and financial protection is insufficient to enable effective UHC. Quality assurance and improvement need to work in tandem with the SDGs goal of achieving UHC. As yet, evidence and research on the quality outcomes of various financial and policy strategies employed in pursuing UHC at scale are still deficient, but several interventions have proven successful in specific
contexts. The following illustrative strategies and interventions have been highlighted in this chapter:
- A maternity care experiment in India indicated that input and output incentive contracts resulted in a more than 20 percent reduction in PPH.
- mHealth interventions can be effective and have improved the accuracy of data submission by health workers, improved clinical decision-making skills, and had positive effects on NCDs (although caution is needed to ensure person-centeredness).
- Clinical decision support is feasible to implement and accepted by providers, improves work flow, and is cost-effective.
- Demand creation at the community level was a successful strategy for improving the uptake of antenatal services, but it was most effective in reducing rates of stillbirth when coupled with supply-side efforts to improve the quality of care and system strength.
Overall, the studies reviewed on accreditation also provide a growing base of evidence that this strategy can create a safety and quality culture, in addition to yielding real improvements in health outcomes:
- Accreditation status in Brazil was significantly associated with patient safety and quality management activities.
- Accredited hospitals compared with nonaccredited hospitals in Jordan saw decreased rates of next-day readmission to the intensive care unit, reduced staff turnover, and increased medical record completion.
- Accredited providers and institutions in the Philippines scored higher than nonaccredited facilities.
- Accredited health centers in Egypt had higher patient and provider satisfaction and performed better on patients’ rights, information systems, compliance with care standards, and recording of patient visits in records.
The committee wishes again to emphasize the importance of context and culture in all quality interventions, and although the above examples show many successes, they may not be easily translated to another country or institutional environment. We urge health system and country leaders to employ the design principles outlined in Chapter 2 when considering these policy and financial levers for improving quality, and hope that additional, tailored research can lead to stronger evidence and greater generalizability for promising interventions.
Conclusion: All countries need to commit to achieving universal quality care to truly realize the benefits of UHC. This commitment will require investment and, equally challenging, changes in culture and beliefs among health care leaders and professionals and the public. It will require rethinking about how to achieve better-quality care in all settings, such as by employing systems thinking, ensuring the reliable use of evidence-based guidelines, fostering innovation in care delivery, empowering the workforce and patients to participate in the improvement of care systems, and building accountability into the system to address collusion and corruption so the system is responsive to and meets the needs of patients. This commitment will also require setting bold aims for ongoing improvement in all domains of quality, and revisiting and updating those aims frequently over time. Finally, since no health system is entirely “public,” partnership and collaboration with the private sector will be necessary to realize this vision and truly improve quality for all citizens.
Recommendation 7-1: Make Accountability for Quality a Top Priority Ongoing improvement of the quality of care in all dimensions should be the daily work and constant responsibility of health care leaders, including, but not limited to, ministries of health. The committee endorses the recent Global Quality report and recommendations of the World Health Organization, the World Bank, and the Organisation for Economic Co-operation and Development, and further recommends the following steps:
- Every ministry of health should develop a national health care quality strategy, together with supporting policies, and should agree to be held accountable for progress.
- Every ministry of health should adopt goals for achieving high-quality care, adapted to their national context, but considering all the dimensions of quality highlighted in this report.
- The United Nations System or a respected global civil society organization should maintain an independent accountability mechanism with which to monitor and report on the progress of nations toward achieving high-quality care.
- Governments, international agencies, and private-sector partners should activate public demand for high quality care through education on patient rights and health literacy, provider choice, measurement, and transparency.
Conclusion: Quality and UHC are not sequential or separate; they are inextricably linked. Without quality, UHC is an empty vessel. Specific
policy levers exist to help embed quality into UHC, but they need to be used as a package of interventions to promote quality improvement. These approaches have not yet shown successful outcomes at scale. As countries move toward UHC, governments will need to use the mechanisms inherent in UHC as levers to accelerate care improvement. These policy levers include, but are not limited to, actively considering quality when making decisions on what services and products to commission or purchase, to whom they will be provided, and how much to pay.
Recommendation 7-2: Use Universal Health Coverage (UHC) as a Lever to Improve the Quality of Care
As ministries of health and health care leaders implement UHC, they should work with payers and providers to improve quality by institutionalizing evidence-based policy levers and systematically assessing their effects on quality. Countries should gather and report on quality metrics in global frameworks and across a range of quality dimensions. Steps within nations should include:
- using financing and coverage mechanisms in UHC that support the provision of high-quality care, such as strategic commissioning and purchasing of services and products, selective contracting, and paying for the value of care;
- carrying out monitoring and evaluation, including clinical audits, community involvement and co-design, and customer satisfaction surveys, to generate data that can be used to ensure that UHC resources are fostering high-quality, continuously improving care; and
- conducting research and evaluation on the impact of policy levers on the quality of care received to improve the evidence base on what interventions lead to better care at a systems level.
REFERENCES
Agyepong, I. A., and S. Adjei. 2008. Public social policy development and implementation: A case study of the Ghana national health insurance scheme. Health Policy Plan 23(2):150–160.
Aitken, M., A. Backliwal, M. Chang, and A. Udeshi. 2013. Understanding healthcare access in India: What is the current state? Parsippany, NJ: IMS Institute for Healthcare Informatics.
Al Tehewy, M., B. Salem, I. Habil, and S. El Okda. 2009. Evaluation of accreditation program in non-governmental organizations’ health units in Egypt: Short-term outcomes. International Journal for Quality in Health Care 21(3):183–189.
Alhassan, R. K., E. Nketiah-Amponsah, N. Spieker, D. K. Arhinful, A. Ogink, P. van Ostenberg, and T. F. Rinke de Wit. 2015. Effect of community engagement interventions on patient safety and risk reduction efforts in primary health facilities: Evidence from Ghana. PLoS One 10(11):e0142389.
Ali, M. K., S. Shah, and N. Tandon. 2011. Review of electronic decision-support tools for diabetes care: A viable option for low- and middle-income countries? Journal of Diabetes Science and Technology 5(3):553–570.
Amon, J. 2015. Dispatches: Stop using hospitals as debtor prisons. Human Rights Watch Dispatches, April 14. https://www.hrw.org/news/2015/04/14/dispatches-stop-using-hospitals-debtor-prisons (accessed June 3, 2018).
Anchala, R., S. Kaptoge, H. Pant, E. Di Angelantonio, O. H. Franco, and D. Prabhakaran. 2015. Evaluation of effectiveness and cost-effectiveness of a clinical decision support system in managing hypertension in resource constrained primary health care settings: Results from a cluster randomized trial. Journal of the American Heart Association 4(1):e001213.
Araj, S. J., and E. Chappy. 2018. Jordan: Health Care Accreditation Council of Jordan: Driving system reform, patient safety, and quality. In Health systems improvement across the globe: Success stories from 60 countries, edited by J. Braithwaite, R. Mannion, Y. Matsuyama, P. Shekelle, S. Whittaker, and S. Al-Adawi. Boca Raton, FL: CRC Press. Pp. 317–324.
Bassuni, E. M., and M. M. Bayoumi. 2015. Improvement critical care patient safety: Using nursing staff development strategies, at Saudi Arabia. Global Journal of Health Science 7(2):335–343.
Bazant, E., S. Sarkar, J. Banda, W. Kanjipite, S. Reinhardt, H. Shasulwe, J. M. Mulilo, and Y. M. Kim. 2014. Effects of a performance and quality improvement intervention on the work environment in HIV-related care: A quasi-experimental evaluation in Zambia. Human Resources for Health 12:73.
Beaubien, J. 2018. How postcards solved the problem of disappearing rice. Goats and Soda: Stories of Life in a Changing World, July 10. https://www.npr.org/sections/goatsandsoda/2018/07/10/627355954/how-postcards-solved-the-problem-of-disappearingrice (accessed July 14, 2018).
Bergh, A. M., S. Baloyi, and R. C. Pattinson. 2015. What is the impact of multi-professional emergency obstetric and neonatal care training? Best Practice & Research: Clinical Obstetrics & Gynaecology 29(8):1028–1043.
Berktas, M., and I. H. Kayral. 2018. Turkey: Establishment of a national healthcare accreditation system. In Health systems improvement across the globe: Success stories from 60 countries, edited by J. Braithwaite, R. Mannion, Y. Matsuyama, P. Shekelle, S. Whittaker, and S. Al-Adawi. Boca Raton, FL: CRC Press. Pp. 279–284.
Berlinger, J. 2016. Hospital investigated after pregnant woman dies. CNN, March 17. https://www.cnn.com/2016/03/17/africa/pregnant-woman-death-cameroon/index.html (accessed August 2, 2018).
Bhutta, Z., G. Darmstadt, R. Haws, M. Yakoob, and J. Lawn. 2009. Delivering interventions to reduce the global burden of stillbirths: Improving service supply and community demand. BMC Pregnancy and Childbirth 9(Suppl. 1):S7. doi:10.1186/1471-2393-9-S1-S7.
Cashin, C., N. Otoo, and K. Toves. 2018. Q&A: What is strategic purchasing for health. https://www.r4d.org/blog/qa-strategic-purchasing-health (accessed July 5, 2018).
Collins, D., U. Saya, and T. Kunda. 2016. The impact of community-based health insurance on access to care and equity in Rwanda. Technical brief. https://www.msh.org/sites/msh.org/files/the_impact_of_cbhi_on_access_to_care_and_equity_in_rwanda.pdf (accessed August 2, 2018).
Das, J., J. Hammer, and K. Leonard. 2008. The quality of medical advice in low-income countries. Journal of Economic Perspectives 22(2):93–114.
Das, J., A. Holla, A. Mohpal, and K. Muralidharan. 2016. Quality and accountability in health care delivery: Audit-study evidence from primary care in India. American Economic Review 106(12):3765–3799.
Devkaran, S., and P. N. O’Farrell. 2015. The impact of hospital accreditation on quality measures: An interrupted time series analysis. BMC Health Services Research 15(1):137.
Duysburgh, E., M. Temmerman, M. Ye, A. Williams, S. Massawe, J. Williams, R. Mpembeni, S. Loukanova, W. E. Haefeli, and A. Blank. 2016. Quality of antenatal and childbirth care in rural health facilities in Burkina Faso, Ghana and Tanzania: An intervention study. Tropical Medicine & International Health 21(1):70–83.
Eichler, R., K. Agarwal, I. Askew, E. Iriarte, L. Morgan, and J. Watson. 2013. Performance-based incentives to improve health status of mothers and newborns: What does the evidence show? Journal of Health, Population and Nutrition 31(4 Suppl. 2):36–47.
Figueras, J., R. Robinson, and E. Jakubowski. 2005. Purchasing to improve health systems performance: Drawing the lessons. In Purchasing to improve health system performance, edited by J. Figueras, R. Robinson, and E. Jakubowski. New York: Open University Press. Pp. 44–82 http://www.euro.who.int/__data/assets/pdf_file/0004/98428/E86300. pdf (accessed August 2, 2018).
Ghana Ministry of Health. 2016. Ghana National Healthcare Quality Strategy (2017–2021). http://www.moh.gov.gh/wp-content/uploads/2017/06/National20Quality20Strategy20Ghana.pdf (accessed June 4, 2018).
Gitobu, C. M., P. B. Gichangi, and W. O. Mwanda. 2018. The effect of Kenya’s free maternal health care policy on the utilization of health facility delivery services and maternal and neonatal mortality in public health facilities. BMC Pregnancy Childbirth 18(1):77.
Goldfarb, N. I., V. Maio, C. T. Carter, L. Pizzi, and D. B. Nash. 2003. How does quality enter into health care purchasing decisions? New York: The Commonwealth Fund.
Gottret, P., and G. Schieber. 2006. Health financing revisited: A practitioner’s guide. Washington, DC: World Bank.
Govindarajan, V., and R. Ramamurti. 2013. Delivering world-class health care, affordably. Harvard Business Review, November. https://hbr.org/2013/11/delivering-world-class-health-care-affordably (accessed June 4, 2018).
Gunatilleke, G. 2009. Negotiating development in an evolving democracy: Lessons from Sri Lanka. Harvard Asia Pacific Review.
Guo, M. 2017. Meet the digitally savvy Chinese patients. https://cn-en.kantar.com/business/health/2017/meet-the-digitally-savvy-chinese-patients (accessed June 4, 2018).
Halasa, Y. A., W. Zeng, E. Chappy, and D. S. Shepard. 2015. Value and impact of international hospital accreditation: A case study from Jordan. Eastern Mediterranean Health Journal 21(2):90–99.
Hanson, K., L. Gilson, C. Goodman, A. Mills, R. Smith, R. Feachem, N. S. Feachem, T. P. Koehlmoos, and H. Kinlaw. 2008. Is private health care the answer to the health problems of the world’s poor? PLoS Medicine 5(11):e233.
Hercot, D., B. Meessen, V. Ridde, and L. Gilson. 2011. Removing user fees for health services in low-income countries: A multi-country review framework for assessing the process of policy change. Health Policy Plan 26(Suppl. 2):ii5–ii15.
Hudson, S., and R. V. Rikard. 2018. The case for health literacy: Moving from equity to liberation. Washington, DC: National Academy of Medicine.
Indian Ministry of Health and Family Welfare. 2017. Draft patient safety implementation framework. https://mohfw.gov.in/newshighlights/draft-patients-safety-implementation-framework (accessed June 4, 2018).
IOM (Institute of Medicine). 2004. Health literacy: A prescription to end confusion. Washington, DC: The National Academies Press.
Kalisa, I. R., S. F. Musange, D. Collins, U. Saya, and T. Kunda. 2015. The development of community-based health insurance in Rwanda—experiences and lessons. Medford, MA: University of Rwanda College of Medicine and Health Sciences School of Public Health, Kigali, Rwanda and Management Sciences for Health.
Kallander, K., J. K. Tibenderana, O. J. Akpogheneta, D. L. Strachan, Z. Hill, A. H. ten Asbroek, L. Conteh, B. R. Kirkwood, and S. R. Meek. 2013. Mobile health (mHealth) approaches and lessons for increased performance and retention of community health workers in low- and middle-income countries: A review. Journal of Medical Internet Research 15(1):e17. doi:10.2196/jmir.2130.
Karan, A., W. Yip, and A. Mahal. 2017. Extending health insurance to the poor in India: An impact evaluation of Rashtriya Swasthya Bima Yojana on out of pocket spending for healthcare. Social Science & Medicine (1982) 181:83–92. doi:10.1016/j. socscimed.2017.03.053.
Lagomarsino, G., S. Nachuk, and S. S. Kundra. 2009. Public stewardship of private providers in mixed health systems: Synthesis report from The Rockefeller Foundation-sponsored initiative on the role of the private sector in health systems in developing countries. Washington, DC: The Rockefeller Foundation. https://www.r4d.org/wp-content/uploads/Public-Stewardship-of-Private-Providers-in-Mixed-Health-Systems.pdf (accessed June 4, 2018).
Leatherman, S., D. Berwick, D. Iles, L. S. Lewin, F. Davidoff, T. Nolan, and M. Bisognano. 2003. The business case for quality: Case studies and an analysis. Health Affairs 22(2):17–30.
Limwattananon, S., S. Neelsen, O. O’Donnell, P. Prakongsai, V. Tangcharoensathien, and E. van Doorslaer. 2013. Universal coverage on a budget: Impacts on health care utilization and out-of-pocket expenditures in Thailand. Munich, Germany: CESifo Group Munich.
Liu, C., X. Zhang, and J. Wan. 2015. Public reporting influences antibiotic and injection prescription in primary care: A segmented regression analysis. Journal of Evaluation in Clinical Practice 21(4):597–603.
Liu, C., X. Zhang, X. Wang, X. Zhang, J. Wan, and F. Zhong. 2016. Does public reporting influence antibiotic and injection prescribing to all patients? A cluster-randomized matched-pair trial in China. Medicine (Baltimore) 95(26):e3965.
Maia, J. X., L. A. de Sousa, M. S. Marcolino, C. S. Cardoso, J. L. da Silva, M. B. Alkmim, and A. L. Ribeiro. 2016. The impact of a clinical decision support system in diabetes primary care patients in a developing country. Diabetes Technology & Therapeutics 18(4):258–263.
Mate, K. S., Z. K. Sifrim, K. Chalkidou, F. Cluzeau, D. Cutler, M. Kimball, T. Morente, H. Smits, and P. Barker. 2013. Improving health system quality in low- and middle-income countries that are expanding health coverage: A framework for insurance. International Journal for Quality in Health Care 25(5):497–504.
McKinsey’s Health Systems and Services Practice. 2011. Driving down the costs of high-quality care: Lessons from the Aravind Eye Care system. https://www.mckinsey.com/~/media/mckinsey/dotcom/client_service/Healthcare%20Systems%20and%20Services/Health%20International/Issue%2011%20new%20PDFs/HI11_18%20AravindEyeCareSys_noprint.ashx (accessed July 10, 2018).
Mensah, N., F. Sukums, T. Awine, A. Meid, J. Williams, P. Akweongo, J. Kaltschmidt, W. E. Haefeli, and A. Blank. 2015. Impact of an electronic clinical decision support system on workflow in antenatal care: The QUALMAT eCDSS in rural health care facilities in Ghana and Tanzania. Global Health Action 8:25756.
Miller, G., and K. S. Babiarz. 2013. Pay-for-performance incentives in low- and middle-income country health programs. Working paper series no. 18932. Cambridge, MA: National Bureau of Economic Research. http://www.nber.org/papers/w18932 (accessed August 2, 2018).
Miller, G., R. Luo, L. Zhang, S. Sylvia, Y. Shi, P. Foo, Q. Zhao, R. Martorell, A. Medina, and S. Rozelle. 2012. Effectiveness of provider incentives for anaemia reduction in rural China: A cluster randomised trial. British Medical Journal 345:e4809.
Missoni, E. 2010. Attaining universal health coverage: A research initiative to support evidence based advocacy and policy making. Milan, Italy: Global Health Group, Cergas Bocconi University.
Mohanan, M., G. Miller, and Y. Truskinovsky. 2017. Different strokes for different folks: Experimental evidence on the effectiveness of input and output incentive contracts for health care providers with different levels of skills. https://www.cgdev.org/sites/default/files/different-strokes-different-folks.pdf (accessed August 2, 2018).
Morton, M., S. Nagpal, R. Sadanandan, and S. Bauhoff. 2016. India’s largest hospital insurance program faces challenges in using claims data to measure quality. Health Affairs 35(10):1792–1799.
Ng, G. K., G. K. Leung, J. M. Johnston, and B. J. Cowling. 2013. Factors affecting implementation of accreditation programmes and the impact of the accreditation process on quality improvement in hospitals: A SWOT analysis. Hong Kong Medical Journal 19(5):434–446.
Nimpagaritse, M., and M. P. Bertone. 2011. The sudden removal of user fees: The perspective of a frontline manager in Burundi. Health Policy Plan 26(Suppl. 2):ii63–ii71.
Okungu, V. 2015. Towards universal health coverage: Exploring healthcare-related financial risk protection for the informal sector in Kenya. Dissertation. Cape Town, South Africa: University of Cape Town.
Okungu, V., J. Chuma, S. Mulupi, and D. McIntyre. 2018. Extending coverage to informal sector populations in Kenya: Design preferences and implications for financing policy. BMC Health Services Research 18(1):13.
Otremba, M., G. Berland, and J. J. Amon. 2015. Hospitals as debtor prisons. The Lancet Global Health 3(5):e253–e254.
Peabody, J. W., S. A. Quimbo, R. Shimkhada, K. Woo, and O. Solon. 2008. Should we have confidence if a physician is accredited? A study of the relative impacts of accreditation and insurance payments on quality of care in the Philippines. Social Science & Medicine (1982) 67(4):505–510.
Ravi, S., and N. Sood. 2018. Is the national health policy protection scheme good public policy? Brookings, March 12. https://www.brookings.edu/opinions/is-the-national-health-protection-scheme-good-public-policy (accessed June 4, 2018).
Republic of Rwanda. 2010. Rwanda community based health insurance policy. Kigali, Rwanda: Ministry of Health.
Saut, A. M., F. T. Berssaneti, and M. C. Moreno. 2017. Evaluating the impact of accreditation on Brazilian healthcare organizations: A quantitative study. International Journal for Quality in Health Care 29(5):713–721.
Singh, P. 2011. Performance pay and information: Reducing child malnutrition in urban slums. Munich, Germany: University Library of Munich.
Sood, N., and Z. Wagner. 2013. For-profit sector immunization service provision: Does low provision create a barrier to take-up? Health Policy Plan 28(7):730–738.
Sood, N., and Z. Wagner. 2018. Social health insurance for the poor: Lessons from a health insurance programme in Karnataka, India. BMJ Global Health 3(1).
Spreng, C. P., I. P. Ojo, N. E. Burger, N. Sood, J. W. Peabody, and L. M. Demaria. 2014. Does stewardship make a difference in the quality of care? Evidence from clinics and pharmacies in Kenya and Ghana. International Journal for Quality in Health Care 26(4):388–396.
Starfield, B., L. Shi, and J. Macinko. 2005. Contribution of primary care to health systems and health. http://www.commonwealthfund.org/usr_doc/Starfield_Milbank.pdf (accessed June 4, 2018).
Stephani, V., D. Opoku, and W. Quentin. 2016. A systematic review of randomized controlled trials of mHealth interventions against non-communicable diseases in developing countries. BMC Public Health 16(1):572.
Stuckler, D., A. B. Feigl, S. Basu, and M. McKee. 2010. The political economy of universal health coverage. Paper presented at Global Symposium on Health Systems Research, Montreux, Switzerland. http://www.pacifichealthsummit.org/downloads/UHC/the%20political%20economy%20of%20uhc.PDF (accessed June 4, 2018).
Sunmonu, F. 2017. PurpleSource healthcare. http://www.nationalacademies.org/hmd/~/media/Files/Activity%20Files/Global/GlobalQualityofCare/Meeting%202/Presentations/Sunmonu%20PurpleSource.pdf (accessed December 20, 2017).
Suthar, A. B., J. M. Nagata, S. Nsanzimana, T. Bärnighausen, E. K. Negussie, and M. C. Doherty. 2017. Performance-based financing for improving HIV/AIDS service delivery: A systematic review. BMC Health Services Research 17:6.
Tang, Y., C. Liu, and X. Zhang. 2016. Public reporting as a prescriptions quality improvement measure in primary care settings in China: Variations in effects associated with diagnoses. Scientific Reports 6.
Tangcharoensathien, V., W. Patcharanarumol, Chitpranee, P. Prakongsai, P. Jongudomsuk, S. Srithamrongsawat, and J. Thammathataree. 2010. Thailand health financing review 2010. Bangkok, Thailand: WHO South East Asia Regional Office.
Taylor, A., E. Escobar, and K. Udayakumar. 2017. Expanding access to low-cost, high-quality tertiary care. https://www.commonwealthfund.org/publications/case-study/2017/nov/expanding-access-low-cost-high-quality-tertiary-care (accessed July 10, 2018).
The Economist. 2018. The price of human lives: More and wiser health-care spending could save millions of lives. https://www.economist.com/special-report/2018/04/26/more-and-wiser-health-care-spending-could-save-millions-of-lives (accessed May 18, 2018).
Upneja, A. 2015. India: Examining the efficacy of the RSBY program in providing healthcare for the rural poor. Yale Global Health Review, October 5. https://yaleglobalhealthreview.com/2015/10/05/india-examining-the-efficacy-of-the-rsby-program-in-providing-healthcare-for-the-rural-poor (accessed June 4, 2018).
Vasan, A., D. C. Mabey, S. Chaudhri, H. A. Brown Epstein, and S. D. Lawn. 2017. Support and performance improvement for primary health care workers in low- and middle-income countries: A scoping review of intervention design and methods. Health Policy Plan 32(3):437–452.
Wagner, Z., M. Shah, and N. Sood. 2015. Barriers to use of oral rehydration salts for child diarrhea in the private sector: Evidence from India. Journal of Tropical Pediatrics 61(1):37–43.
Wee, S.-L. 2018. Want to see your baby? In China, it can cost you. The New York Times, May 22. https://www.nytimes.com/2018/05/22/business/china-baby-money-hospital.html (accessed June 4, 2018).
WHO (World Health Organization). 2005. Distribution of health payments and catastrophic expenditures: Methodology. Geneva, Switzerland: WHO.
WHO. 2010. The World Health Report: Health systems financing; the path to universal coverage. Geneva, Switzerland: WHO.
WHO. 2018a. Handbook for national quality policy and strategy: A practical approach for developing policy and strategy to improve quality of care. Geneva, Switzerland: WHO.
WHO. 2018b. Handbook for national quality policy and strategy: A practical approach for developing policy and strategy to improve quality of care. Geneva, Switzerland: WHO. License: CC BY-NC-SA 3.0 IGO.
WHO and World Bank. 2017. Tracking universal health coverage: 2017 global monitoring report. Washington, DC: WHO and World Bank.
WHO, OECD (Organisation for Economic Co-operation and Development), and World Bank. 2018. Delivering quality health services: A global imperative for universal health coverage. Geneva, Switzerland: WHO, OECD, and World Bank.
Wickham, S., D. Feeley, E. E. Ajoku, O. Filani, J. Arrieta, C. Ternes, S. Narino, O. S. Gonzalez, H. Magge, A. Kiflie, A. S. Esteifanos, N. Tweneboa, P. Amofah, and E. Asiedu. in press. National quality strategy case studies: Learning from Ethiopia, Ghana, Mexico, Nigeria, and Scotland. Boston, MA: Institute for Healthcare Improvement.
Witter, S., A. Fretheim, F. L. Kessy, and A. K. Lindahl. 2012. Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database of Systematic Reviews (2):CD007899. doi:10.1002/14651858.CD007899. pub2.
World Bank. 2016a. Financing. http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTHEALTHNUTRITIONANDPOPULATION/EXTHSD/0,,contentMDK:22523961~menuPK:376799~pagePK:148956~piPK:216618~theSitePK:376793,00.html (accessed July 10, 2018).
World Bank. 2016b. UHC in Africa: A framework for action. Washington, DC: World Bank.
World Bank. 2018. Current health expenditure per capita (current US$). https://data.worldbank.org/indicator/SH.XPD.CHEX.PC.CD (accessed July 10, 2018).
Xu, K., D. B. Evans, G. Carrin, A. M. Aguilar-Rivera, P. Musgrove, and T. Evans. 2007. Protecting households from catastrophic health spending. Health Affairs 26(4):972–983.
Xu, K., P. Saksena, M. Jowett, C. Indikadahena, J. Kutzin, and D. B. Evans. 2010. Exploring the thresholds of health expenditure for health protection against financial risk. Geneva, Switzerland: WHO.
Xu, K., A. Soucat, J. Kutzin, C. Brindley, E. Dale, N. Van de Maele, T. Roubal, Chandika Indikadahena, H. Toure, and V. Cherilova. 2018. New perspectives on global health spending for universal health coverage. Geneva, Switzerland: WHO.
Yang, L., C. Liu, L. Wang, X. Yin, and X. Zhang. 2014. Public reporting improves antibiotic prescribing for upper respiratory tract infections in primary care: A matched-pair cluster-randomized trial in China. Health Research Policy and Systems 12:61. doi:10.1186/1478-4505-12-61.
Yates, R., T. Brookes, and E. Whitaker. 2017. Hospital detentions for non-payment of fees: A denial of rights and dignity. London, UK: Chatham House, Centre on Global Health Security.
Zhang, X., L. Wang, and X. Zhang. 2014. Application of propensity scores to explore the effect of public reporting of medicine use information on rational drug use in China: A quasi-experimental design. BMC Health Services Research 14:492.
This page intentionally left blank.










































