
8
Implementing the Committee’s Recommendations to Improve Public Health
Improving public health requires the use of multifaceted approaches to emerging health issues. In environmental health—the subset of public health focused on environmental factors—mitigation of potential harms associated with chemical exposures is often complicated because there is no exposure surveillance system for most chemicals. To address per- and polyfluoroalkyl substances (PFAS) effectively as a public health issue, it will be important to identify the people and communities with high exposures to PFAS, improve environmental health education for both clinicians and the public, and prevent exposures. Thus, the committee’s recommendations would be most effective if implemented as part of a larger national effort toward increased PFAS-focused biomonitoring, exposure surveillance, and education around environmental health.
To promote a coordinated response to PFAS exposures, the committee makes the following recommendations:
Recommendation 8-1: Laboratories conducting PFAS testing of serum or plasma should report the results to state public health authorities, following the respective states’ statutes and reporting regulations. This reporting would improve PFAS exposure surveillance; it could be linked with the Centers for Disease Control and Prevention’s environmental public health tracking network and help build capacity for improvements in the state-based national biomonitoring network.
BIOMONITORING AND SURVEILLANCE
PFAS exposure is nearly ubiquitous, but individual levels of exposure are not consistently measured or documented (CDC, 2021; NASEM, 2020, 2021a). Given the persistence of most PFAS in the human body, biomonitoring will likely produce meaningful exposure data, especially for those PFAS with longer half-lives. Collecting these data is critical to identifying communities and other areas with elevated PFAS exposure. Failing to identify such communities magnifies existing disparities for those that already have limited access to health care, live in areas of high exposure, and do not know that they may be at elevated risk for PFAS-associated health outcomes. Using biomonitoring data to establish exposure surveillance programs while also ensuring that medical professionals and the public have access to clear, accurate information about the risks of PFAS exposure will improve public health overall while also empowering people and communities to safeguard their own health.
According to the 2006 report by the National Research Council Human Biomonitoring for Environmental Chemicals:
Identifying, controlling, and preventing population exposures to potentially harmful environmental chemicals have been cornerstones of U.S. environmental health efforts. Biomonitoring has become a tool that is central to these efforts. (NRC, 2006, p. 1)
While aggregate PFAS biomonitoring data can be used to promote population health, individual PFAS biomonitoring can provide people with information about their personal exposures, which is
important in informing clinical care (see Chapter 5). Therefore, access to PFAS blood tests for patients likely to have a history of elevated exposure as well as the results of those tests can help individuals better understand and, if possible, address their personal risk from PFAS exposure. Additionally, while biomonitoring studies are important to identify exposed communities and study potential health outcomes, PFAS testing intended to inform an individual’s medical care should be coordinated by clinicians to ensure appropriate care and follow-up.
Improving access to PFAS blood testing for individuals could also allow for the collection of aggregate biomonitoring data if the results were compiled into a database. As discussed in Chapter 5, public health professionals can use those data to determine reference ranges of PFAS exposure in the general population. Understanding those ranges of exposure would support prioritization and allocation of funding and resources for preventive medicine or public health actions. Other high-profile cases demonstrate this powerful use of biomonitoring data to improve public health practice, as occurred in 2015 when Dr. Mona Hanna-Attisha began reviewing her patients’ medical records and realized that the percentage of patients with elevated blood lead levels had increased after the city of Flint, Michigan, changed its water source.1
In addition to informing clinical care, biomonitoring data can be used in establishing exposure surveillance programs. Biomonitoring-based exposure surveillance enables public health practitioners and policy makers to identify exposure trends, mitigate ongoing exposures, and study associations between exposures and disease outcomes (Goldman et al., 1995; Thacker et al., 1996). In contrast with agencies’ ongoing monitoring of environmental contaminants in air, soil, and water, there are few comprehensive databases or collection strategies for measuring and tracking levels in exposed people (Latshaw et al., 2017). The data that are currently collected, such as measurements from the National Health and Nutrition Examination Survey (NHANES),2 often provide a snapshot of exposure that is useful in tracking nationwide trends in exposure over time, but cannot inform a localized public health response or help identify potential exposure “hot spots.” Additionally, unlike the National Health Interview Survey,3 the NHANES does not list urban versus rural as a publicly available variable, which limits researchers’ ability to identify potential location-based disparities in PFAS exposure. Without collecting and compiling comprehensive PFAS biomonitoring data, federal agencies are less able to prioritize highly exposed communities in their mitigation strategies. Additionally, a lack of biomonitoring data limits studies on putative health effects, resulting in continued uncertainty that hinders public health response. As Kristen Mello stated during the committee’s April 7, 2021, town hall, “Don’t avoid taking our data and then complain about data gaps.”
An effective strategy for PFAS exposure surveillance would involve multiple levels of public health response (Colles et al., 2021; Eatman and Strosnider, 2017). As with U.S. programs on pediatric monitoring for lead exposure, laboratories would report the biomonitoring results, zip code, and demographic information to state health departments, which in turn would report the data to the federal government. Data collected by states could be more geographically granular than the data typically accessible through NHANES, thereby enabling localized public health responses for highly contaminated areas (Nassif et al., 2021). Additionally, hierarchical data collection and reporting processes might include repeated stopgaps and promote oversight to ensure that clinicians, researchers, and public health agencies were using the data as effectively as possible.
ENVIRONMENTAL HEALTH EDUCATION
If the use of biomonitoring data and environmental surveillance programs is to be most effective at preventing or at least minimizing clinical disease associated with exposure, clinicians and the public
___________________
1 See ww.npr.org/sections/health-shots/2018/06/25/623126968/pediatrician-who-exposed-flint-water-crisisshares-her-story-of-resistance (accessed June 17, 2022).
2 See https://www.cdc.gov/nchs/nhanes/index.htm (accessed June 17, 2022).
3 See https://www.cdc.gov/nchs/nhis (accessed June 17, 2022).
must have access to the information and know what to do with it. From a clinical perspective, providers need a better working knowledge of environmental health and chemical exposures. At the committee’s town halls, speakers described their frustration with trying to obtain medical care from practitioners who were unfamiliar with PFAS and did not understand the environmental health contexts of the communities in which they practiced. At the town hall on April 7, 2021, Hope Grosse said:
When I would go to the doctors and tell them about some of the exposures of over 50 chemicals that I was exposed to, the doctors would laugh and say no. Clearly, they didn’t have any information about environmental components [of disease]. They made me feel small; they made me feel stupid and embarrassed even just asking the question.
The National Academies has previously acknowledged the issue of limited clinical education in environmental health. The 1991 Institute of Medicine (IOM) report Addressing the Physician Shortage in Occupational and Environmental Medicine: Report of a Study notes that all levels of medical education, from undergraduate to graduate and continuing education programs, provide limited, if any, training in occupational and environmental medicine. The report recommends that occupational and environmental medicine concepts be introduced early and continuously during medical education (IOM, 1991). Likewise, Environmental Medicine: Integrating a Missing Element into Medical Education notes a need for more environmentally literate physicians (IOM, 1995a). Decades later, however, Green-McKenzie and colleagues (2021) found that only 70 percent of medical students had heard of occupational and environmental medicine, and most of them had received only one lecture on the topic. After medical school, residency programs align with specialty requirements, which may not include further training in environmental and occupational medicine. In addition to the more formal medical training doctors receive in medical school and residency programs, professional associations such as the American Medical Association,4 the American College of Preventive Medicine,5 and the American College of Occupational and Environmental Medicine6 offer continuing medical education modules on environmental health. However, these modules are optional, meaning that physicians may not learn about environmental and occupational medicine after medical school, either.
Physicians are not alone in their limitations with respect to environmental health education. According to the 1995 IOM report Nursing, Health, and the Environment: Strengthening the Relationship to Improve the Public’s Health, “environmental health currently receives scant attention in nursing education and research” (IOM, 1995b, p. 14). The report calls for more nurses with education in environmental health, given that nurses represent the largest proportion of the health care workforce. Similarly, a recent commentary on the nursing profession notes that most nurses do not see themselves as environmental health practitioners or scientists (McCauley and Hayes, 2021). To address this shortcoming, environmental health is now a recommended domain for nursing education (NASEM, 2021b); in addition, nurses may need additional continuing education on environmental health topics.
Continuing education of clinicians is important to address knowledge gaps in environmental health. Increasing the opportunities for clinician education in environmental and occupational medicine; promoting collaborative, interdisciplinary environmental health networks; and framing environmental health as a tenet of preventive medicine and primary care are essential to ensure proper medical care for those facing environmental exposures and to assist families in reducing exposures when possible. One resource that can be leveraged to help respond to environmental exposures is the Pediatric Environmental Health Specialty Units (PEHSUs). ATSDR funds the PEHSUs with support from EPA. The PEHSUs are a “national network of experts in the prevention, diagnosis, management, and treatment of health issues that arise from environmental exposures from preconception through adolescence.”7 While the primary
___________________
4 See https://www.ama-assn.org (accessed June 17, 2022).
5 See https://www.acpm.org (accessed June 17, 2022).
6 See https://acoem.org (accessed June 17, 2022).
7 See https://pehsu.net (accessed July 27, 2022).
focus is reproductive and children’s health, clinicians will work with the whole family in determining exposure pathways and reducing these exposures. The PEHSU network includes nurses, physicians, medical toxicologists, and public health professionals and promotes collaboration among these diverse groups of practitioners. The network provides continuing education opportunities and information on PFAS for both health care professionals and community members. PEHSU-affiliated practitioners have proposed concrete environmental health competency areas for medical education programs (Goldman et al., 2021). Similarly, the Alliance of Nurses for Healthy Environments (ANHE)8 addresses environmental exposures and health, including PFAS and related clinical care, in various online resources and engages with universities to integrate environmental health into their nursing education curricula. Other organizations, such as the Children’s Environmental Health Network,9 also provide educational materials in environmental health for health care providers.
Many public health practitioners have received training in environmental health because until recently, it was a required component of master of public health (M.P.H.) programs; however, the curriculum for public health is changing. In 2016, the Council on Education for Public Health (CEPH) released new accreditation criteria, aimed at offering schools of public health greater flexibility in course offerings and students a more applied, practice-based education.10 With these more flexible coursework requirements, the CEPH removed the explicit requirement for education in environmental health sciences, replacing it and the other core disciplines with a series of competencies. This change may inadvertently lead to reduced environmental health training for public health professionals.11 Indeed, by December 2019, just 91 percent of accredited M.P.H. programs continued to offer a concentration in environmental health sciences.12 Addressing such challenges as PFAS requires a public health workforce with competency in environmental health sciences, toxicology, and epidemiology, which is why the Association for Prevention Teaching and Research calls on schools and programs in public health to maintain existing environmental health content and develop such content if previously eliminated or never offered (Levy et al., 2022).13
The public’s environmental health literacy complements clinician education in environmental health by promoting individuals’ personal health decision making while galvanizing communities to demand population-level public health responses. Historically, health literacy as a concept centered on individual decision making based on an understanding of health information. In Healthy People 2030, however, the U.S. Department of Health and Human Services (HHS) expanded the definition to encompass organizations’ responsibility to ensure that individuals have access, understanding, and services to inform their health decisions, a concept HHS refers to as organizational health literacy.14
The term health literacy as used in this report focuses on Nutbeam’s (2000) second and third levels of health literacy—interactive and critical literacy—which emphasize empowerment, autonomy, and action. More specifically, National Institute of Environmental Health Sciences (NIEHS) authors Finn and O’Fallon (2017) describe environmental health literacy as
a philosophical perspective, a public health policy to improve literacy and health literacy in the general public, and a set of strategies to empower individuals and communities to exert control over the environmental exposures that may lead to adverse health outcomes. (p. 495)
___________________
8 See https://envirn.org (accessed June 17, 2022).
9 See https://cehn.org (accessed June 17, 2022).
10 See https://media.ceph.org/documents/Environmental_Health.pdf (accessed June 17, 2022).
11 See http://www.publichealthnewswire.org/?p=environmental-health-in-education (accessed June 17, 2022).
12 See https://media.ceph.org/documents/Environmental_Health.pdf (accessed June 17, 2022).
13 See https://www.aptrweb.org/page/ClimateChange (accessed June 17, 2022).
14 See https://health.gov/healthypeople/priority-areas/health-literacy-healthy-people-2030/history-health-literacydefinitions (accessed June 17, 2022).
Building on the concept of health literacy, environmental health literacy has three dimensions: (1) awareness and knowledge of an environmental exposure, (2) skills and self-efficacy that allow individuals to make decisions to protect their own health, and (3) community change based on actions that reduce environmental exposures and protect public health (Gray, 2018). The committee recognizes that many exposures to PFAS are beyond individual control, and placing the onus for action on individuals often imposes an undue burden. Nevertheless, environmental health literacy can empower people to understand their own risks and ask their providers informed questions. As demonstrated by the community liaisons and town hall speakers who contributed to this study, many individuals have already worked especially hard to access information and educate themselves on PFAS.
In keeping with the principle of reducing the burden on exposed community members, PFAS-related environmental health literacy should center on making PFAS research publicly available and understandable for general audiences. Open access publication platforms are more accessible than those that are behind paywalls. Summaries written in plain language for the lay public, as blogs, news articles, and podcasts would be even better for increasing awareness about PFAS. Such resources as ATSDR’s ToxFAQs15; Northeastern University’s PFAS-TOX Database16; the PFAS Research, Education, and Action for Community Health PFAS Exchange17; and the Environmental Working Group’s PFAS Contamination in the U.S. map18 distill key information for the public and may serve as models for other environmental health literacy work. Other online resources, such as Purdue University’s Online Writing Lab, describe considerations for evaluating the credibility of online sources that can serve as a guide for both those developing and those using the resources.19 People must have access to information that can help them make health decisions and advocate for the health of their communities.
BARRIERS TO IMPLEMENTATION
Barriers to the committee’s proposed implementation approach include difficulties with PFAS testing, lack of data standardization, poor coordination among experts from different disciplines, and a lack of funding for and availability of education in environmental and occupational medicine and environmental health literacy activities. Few laboratories currently have the capability to test for PFAS. The testing methodology is complex, and not all PFAS can be detected in serum or plasma. Data standardization is also a challenge (Latshaw et al., 2017) given the variability in testing methods, participant demographics, and exposure sources. As noted in Chapter 5 of this report, PFAS testing is expensive, and limiting the availability of testing based on access to consistent clinical care and insurance coverage could exacerbate health disparities in exposed communities. Furthermore, comprehensive PFAS exposure surveillance requires collaboration among a range of experts across different fields (Nassif et al., 2021); training in environmental and occupational medicine and environmental health is lacking; and support for PFAS health literacy is limited.
Given widespread PFAS exposure and the putative health effects associated with these chemicals, public health authorities would do well to prioritize addressing these barriers. Laboratory capacity to test for PFAS could be increased through coordination with the Association of Public Health Laboratories. Biomonitoring data and exposure surveillance programs could be standardized as long as they were developed with structures in place to ensure that the data were collected with the intent of their being comparable. The Network Steering Committee of the National Biomonitoring Network provides a template for successful implementation (Nassif et al., 2021).
___________________
15 See https://wwwn.cdc.gov/TSP/ToxFAQs/ToxFAQsLanding.aspx (accessed June 17, 2022).
16 See https://pfasproject.com/pfas-toxic-database (accessed June 17, 2022).
17 See https://pfas-exchange.org (accessed June 17, 2022).
18 See https://www.ewg.org/interactive-maps/pfas_contamination/map (accessed June 17, 2022).
19 See https://owl.purdue.edu/owl/research_and_citation/conducting_research/evaluating_sources_of_information/evaluating_digital_sources.html (accessed June 17, 2022).
Finally, continuing education opportunities such as “train-in-place” programs allow clinicians to learn environmental and occupational medicine concepts during the course of their ongoing practice (Green-McKenzie et al., 2021). Optimizing these programs and other innovative education strategies, as well as planning communication efforts as part of biomonitoring studies (NRC, 2006), can increase environmental health knowledge without requiring unattainable funding allocations.
MOVING FORWARD
Based on the recommendations and conclusions of this report, ATSDR, NIEHS, environmental health organizations, and bodies responsible for clinical education can take specific actions to address issues of PFAS contamination and clinical care, which will ultimately lead to improved public health (see Figure 8-1). By updating its PFAS clinical guidance according to the recommendations in Chapter 7, ATSDR will lay the groundwork for clinicians to participate in shared decision making and provide informed care for individuals exposed to PFAS. Access to informed care will allow communities with elevated exposure to PFAS to receive relevant medical advice, testing, screening, and treatment. In addition to improved guidance on clinical care, coordination between ATSDR and the National Biomonitoring Network will allow for the expansion of testing and surveillance. Additional communities identified as having elevated PFAS exposures can then receive informed care.
Additionally, NIEHS can use the information in this report to translate the research gaps identified in Chapter 3 into research needs, prioritizing research on potential associations between PFAS exposure and adverse health outcomes where the evidence is limited. As the research gaps narrow, ATSDR can update its clinical guidance to ensure that clinicians’ knowledge and monitoring of PFAS-associated health outcomes remain current.
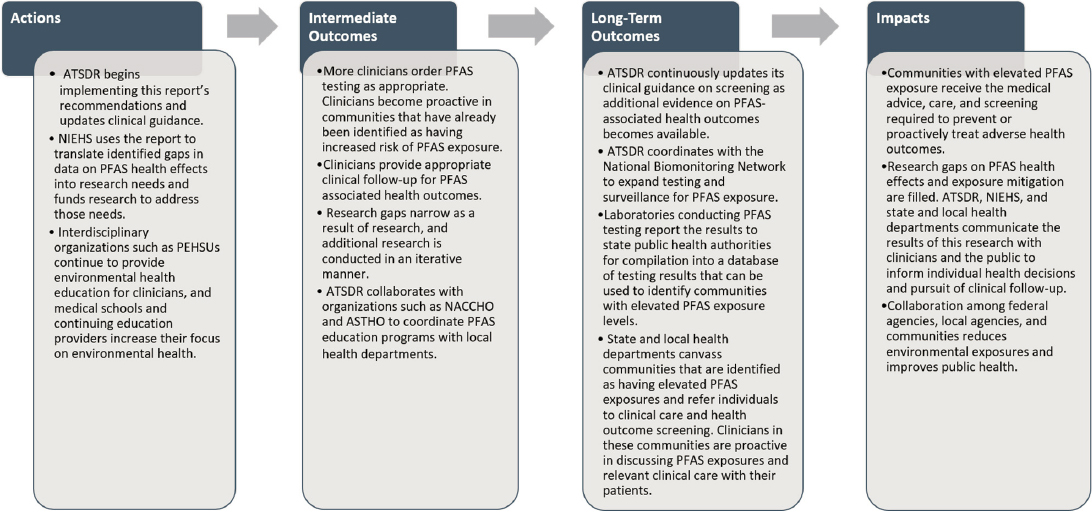
NOTE: ASTHO = Association of State and Territorial Health Officials; ATSDR = Agency for Toxic Substances and Disease Registry; NACCHO = National Association of County and City Health Officials; NIEHS = National Institute of Environmental Health Sciences; PEHSU = Pediatric Environmental Health Specialty Unit.
Environmental health education for clinicians and the public is key to reducing PFAS exposure and ensuring shared decision making and appropriate follow-up. Introductory environmental health training provides the foundation for PFAS-specific clinical education. Given this, the Liaison Committee on Medical Education,20 the Accreditation Council for Graduate Medical Education,21 the American Board of Medical Specialties,22 the Accreditation Commission for Education in Nursing,23 and other bodies responsible for curricula and accreditation of clinician education programs may consider incorporating environmental health into clinician training. Input from such interdisciplinary organizations as PEHSUs and ANHE can support these efforts. State and local health departments may serve as a link between the public and clinicians and proactively provide current information about environmental exposures to the communities they serve. Health departments could receive support for this work through liaison organizations funded by the Centers for Disease Control and Prevention, including the National Association of County and City Health Officials24 and the Association of State and Territorial Health Officials.25 Intentional collaboration at every level—from clinician education; to community partnerships; to local, state, and federal government initiatives—will begin closing the gaps in environmental health infrastructure and training, facilitating the overdue coordinated response and clinical care that people with elevated PFAS exposures deserve.
These efforts in environmental exposure surveillance, environmental health literacy, and improved environmental health tracking will aid in continuing to identify communities impacted by PFAS, which in turn will support exposure mitigation and effective preventive medicine responses. As the committee looks forward, it sees a pressing need for a robust environmental health infrastructure to continue to respond to PFAS, as well as to address other complex emerging and persistent environmental challenges.
REFERENCES
CDC (Centers for Disease Control and Prevention). 2021. Fourth national report on human exposure to environmental chemicals, updated tables. Atlanta, GA: U.S. Department of Health and Human Services. https://www.cdc.gov/biomonitoring/pdf/fourthreport_updatedtables_feb2015.pdf (accessed June 28, 2022).
Colles, A., D. Coertjens, B. Morrens, E. Den Hond, M. Paulussen, L. Bruckers, E. Govarts, A. Covaci, G. Koppen, K. Croes, V. Nelen, N. Van Larebeke, S. De Henauw, T. Fierens, G. Van Gestel, H. Chovanova, M. Mampaey, K. Van Campenhout, I. Loots, W. Baeyens, and G. Schoeters. 2021. Human biomonitoring data enables evidence-informed policy to reduce internal exposure to persistent organic compounds: A case study. International Journal of Environmental Research and Public Health 18(11):5559. https://doi.org/10.3390/ijerph18115559.
Eatman, S., and H. M. Strosnider. 2017. CDC’s National Environmental Public Health Tracking Program in action: Case studies from state and local health departments. Journal of Public Health Management and Practice 23(Suppl 5):S9–S17. https://doi.org/10.1097/phh.0000000000000640.
Finn, S., and L. O’Fallon. 2017. The emergence of environmental health literacy—From its roots to its future potential. Environmental Health Perspectives 125(4):495–501. https://doi.org/10.1289/ehp.1409337.
Goldman, L. R., H. Anton-Culver, M. Kharrazi, and E. Blake. 1995. Banking of human tissue for biomonitoring and exposure assessment: Utility for environmental epidemiology and surveillance. Environmental Health Perspectives 103:31–34. https://doi.org/10.2307/3432557.
___________________
20 See https://lcme.org (accessed June 17, 2022).
21 See https://www.acgme.org (accessed June 17, 2022).
22 See https://www.abms.org (accessed June 17, 2022).
23 See https://www.acenursing.org (accessed June 17, 2022).
24 See https://www.naccho.org (accessed June 17, 2022).
25 See https://www.astho.org (accessed June 17, 2022).
Goldman, R. H., L. Zajac, R. J. Geller, and M. D. Miller. 2021. Developing and implementing core competencies in children’s environmental health for students, trainees, and healthcare providers: A narrative review. BMC Medical Education 21:503. https://doi.org/10.3390/ijerph15030466.
Gray, K. M. 2018. From content knowledge to community change: A review of representations of environmental health literacy. International Journal of Environmental Research and Public Health 15:466. https://doi.org/10.3390/ijerph15030466.
Green-McKenzie, J., U. Savanoor, H. Duran, C. Jones, D. Vearrier, P. Malak, E. Emmett, and F. Shofer. 2021. Outcomes of a survey-based approach to determine factors contributing to the shortage of occupational medicine physicians in the United States. Journal of Public Health Management & Practice 27(3 Suppl):S200–S205. htps://doi.org/10.1097/PHH.0000000000001315.
IOM (Institute of Medicine). 1991. Addressing the physician shortage in occupational and environmental medicine: Report of a study. Washington, DC: National Academy Press. https://doi.org/10.17226/9494.
IOM. 1995a. Environmental medicine: Integrating a missing element into medical education. Washington, DC: National Academy Press. https://doi.org/10.17226/4795.
IOM. 1995b. Nursing, health, and the environment. Washington, DC: National Academy Press. https://doi.org/10.17226/4986.
Latshaw, M. W., R. Degeberg, S. S. Patel, B. Rhodes, E. King, S. Chaudhuri, and J. Nassif. 2017. Advancing environmental health surveillance in the US through a national human biomonitoring network. International Journal of Hygiene and Environmental Health 220(2):98–102.
Levy, C. R., L. M. Phillips, C. J. Murray, L. A. Tallon, and R. M. Caron. 2022. Addressing gaps in public health education to advance environmental justice: Time for action. American Journal of Public Health 112(1):69–74. https://doi.org/10.2105/ajph.2021.306560.
McCauley, L., and R. Hayes. 2021. From Florence to fossil fuels: Nursing has always been about environmental health. Nursing Outlook 69(5):720–731. https://doi.org/10.1016/j.outlook.2021.06.007.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2020. Understanding, controlling, and preventing exposure to PFAS: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/25856.
NASEM. 2021a. Federal government human health PFAS research workshop: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/26054.
NASEM. 2021b. The future of nursing 2020–2030: Charting a path to achieve health equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/25982.
Nassif, J., A. M. Calafat, and K. M. Aldous. 2021. The U.S. national biomonitoring network—Enhancing capability and capacity to assess human chemical exposures. International Journal of Hygiene and Environmental Health 237:113828. https://doi.org/10.1016/j.ijheh.2021.113828.
NRC (National Research Council). 2006. Human biomonitoring for environmental chemicals. Washington, DC: The National Academies Press. https://doi.org/10.17226/11700.
Nutbeam, D. 2000. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International 15(3):259–257. https://doi.org/10.1097/PHH.0000000000001315.
Thacker, S. B., D. F. Stroup, R. G. Parrish, and H. A. Anderson. 1996. Surveillance in environmental public health: Issues, systems, and sources. American Journal of Public Health 86(5):633–638. https://doi.org/10.2105/ajph.86.5.633.








