
6
Guidance for Clinicians on Exposure Determination, PFAS Testing, and Clinical Follow-Up
Despite continued uncertainty about the exact nature of risks from PFAS exposure, clinicians will need to advise and make decisions with patients regarding their exposure. While there is evidence of an association of PFAS with several health outcomes, the likelihood that a particular individual will have any specific adverse health outcome following exposure to PFAS cannot currently be determined with great specificity. There are also gaps in knowledge about how individuals can reduce any potential risks related to PFAS exposure. Despite these gaps, however, many individuals and communities expect clinicians to address PFAS-associated risks as part of routine health care delivery. Although close monitoring and exposure mitigation might prevent or lessen the severity of health effects for those exposed to PFAS, aggressive clinical follow-up could lead to unnecessary treatment, with attendant risk of treatment-related adverse effects; increase patients’ anxiety; and even provide false assurance. For these reasons, trust and clear communication between clinicians and patients are of the utmost importance as they face the task of making decisions that consider all options and incorporate informed preferences, although how best to include children, especially adolescents, in shared decision making is a complicated matter and an active focus of research (Boland et al., 2019). Ongoing and future research should eventually guide clinicians in predicting patient risk and provide an understanding of the benefits and harms of interventions designed to avoid adverse health outcomes.
CRITERIA FOR SCREENING
Screening is the process of testing to identify individuals at high risk for developing a clinical condition or those who have a condition for which signs or symptoms may not be evident. Population screenings are one type of clinical preventive services recommended by health and medical professional agencies and organizations such as the American Academy of Family Physicians (AAFP), the American College of Obstetricians and Gynecologists (ACOG), the American Academy of Pediatrics (AAP), the American Heart Association (AHA), the Health Resources and Services Administration (HRSA), and the U.S. Preventive Services Task Force (USPSTF). These organizations usually recommend population-level screenings as part of routine clinical care when it is clear that they offer a net benefit (compared with potential harms of the screening itself and any subsequent treatment). Although there are different frameworks for determining when to adopt population-level screening, the criteria articulated by Wilson and Jungner (1968) are a common platform for these frameworks:
- The condition should be an important public health concern.
- There should be a treatment for the condition.
- Facilities for diagnosis and treatment should be available.
- There should be a latent stage of the condition.
- There should be a test or examination for the condition.
- The test should be acceptable to the population.
- The natural history of the disease should be adequately understood.
- There should be an agreed-upon policy on whom to treat.
- The total cost of finding a case should be economically balanced in relationship to medical expenditure as a whole.
- Case finding should be a continuous process.
The degree to which these criteria are applied and how they are weighted must be tailored to the particular clinical issue and the perspective of those developing the preventive service. For example, the degree to which the evidence base must be clear can vary based on the urgency of the clinical context, and cost is often not explicitly considered because cost/benefit data from the societal perspective are rarely available. Despite this variation, a key common theme across all frameworks is the need to assess whether the expected benefits of population screening exceed the potential harms. This assessment can be challenging when significant scientific uncertainty exists, as is the case for population screening for PFAS exposure. The committee faced challenges in making population-level recommendations related to the following issues:
- PFAS testing could identify risks for many diverse health outcomes, as opposed to the usual case in which screening identifies one condition or a group of related conditions. Assessment of benefit and harm is difficult if the various potential health outcomes differ in this regard. Furthermore, developing recommendations for clinical follow-up after PFAS exposure is challenging because of the heterogeneity of potential health outcomes.
- The benefits of screening might accrue to individuals other than those who would be screened. For example, determining that an individual had a harmful environmental exposure might not help that person but could lead to broader public health measures that could protect the community.
When there are gaps in knowledge about the benefits and harms of screening or when benefits and harms are closely matched, clinicians should assess individual patient preferences. Informed decision making can be challenging given the above gaps and the limited time clinicians and patients have together. Because standard screening criteria have important limitations in settings of substantial scientific uncertainty, such as PFAS-related health effects, this chapter offers recommendations for basing screening decisions on the principles the committee proposes in Chapter 2.
PFAS-ASSOCIATED HEALTH OUTCOMES
The committee identified several health outcomes associated with PFAS exposure (see Chapter 5). Many are common diseases in the general population, and all have multiple known risk factors (Schrager, 2018). The committee believed it was important to categorize the strength of the evidence for each outcome, but concluded that all conditions with an association should be considered for patient follow-up, as acknowledging the potential risk may make doctors and patients more likely to prioritize screenings. If a patient has a known or suspected exposure to PFAS, the committee encourages clinicians to prioritize screenings for those conditions related to PFAS when relevant and possible. The committee encourages clinicians to use evidence-based best practices and strategies when speaking with patients to support shared decision making and clear health risk communication. Resources such as the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Ambulatory Care Improvement Guide can provide evidence-based trainings, tools, and strategies for shared decision making and clear communication (AHRQ, 2020). The committee did not conduct a meta-analysis to determine the level of increased risk posed by PFAS exposure for each health outcome. Risks vary by exposure level, life stage, and whether patients have other risk factors for developing a health effect. These uncertainties make it infeasible to determine the optimal screening tests and their frequency.
The committee found sufficient evidence of increased risk for the following health outcomes with exposure to PFAS:
- reductions in birthweight;
- dyslipidemia in children and adults;
- kidney cancer in adults; and
- decreased antibody response in children and adults, but with insufficient evidence of an increase in risk or severity of infection or differences in vaccine effectiveness.
The committee found limited suggestive evidence of increased risk for the following health outcomes with exposure to PFAS:
- breast cancer in adults,
- pregnancy-induced hypertension (gestational hypertension and preeclampsia),
- liver enzyme elevations (in children and adults),
- testicular cancer (in adults),
- thyroid dysfunction (in adults), and
- ulcerative colitis (in adults).
For many of these adverse health effects, however, including cancers, it is unclear what clinicians and individuals can do to monitor for their development and intervene to lower the risk related to PFAS exposure. Guidance for clinicians’ engagement in sharing decision making with their patients regarding follow-up care for PFAS-associated health outcomes is included later in this chapter.
Clinical Practice Guidelines for PFAS-Associated Health Outcomes
The committee reviewed clinical practice guidelines for the health effects associated with PFAS exposure, as well as the recommendations from the C-8 Medical Panel (see Table 6-1). The C-8 Medical Panel developed a medical monitoring protocol for a community with high PFAS exposure surrounding Parkersburg, West Virginia. The protocol specifies follow-up for human diseases for which the C-8 Science Panel found a probable link: dyslipidemia, kidney cancer, pregnancy-induced hypertension (gestational hypertension and preeclampsia), testicular cancer, thyroid disfunction, and ulcerative colitis.
Outcomes with Sufficient Evidence of Association
Dyslipidemia in Children and Adults
In the United States, blood testing for lipid and cholesterol levels is recommended throughout the life course based on age and risk factors. AAP recommends that all children be screened once between ages 9 and 11 years and again between 17 and 21 years, with selective screening for children over 2 years of age with a family history of lipid and cholesterol disorders or heart disease (Richerson et al., 2017). AHA recommends screening every 4–6 years for people aged 20 or older who are at low risk for cardiovascular disease (Grundy et al., 2019). The C-8 Medical Panel provided cholesterol screening starting as early as 2 years of age, which is similar to the age recommended for cholesterol screening for children with a family history of lipid disorders (C-8 Medical Panel, 2013).
Reductions in Birthweight
Birthweight is an important and well-established pregnancy outcome. Clinical prevention guidance for reductions in birthweight is to screen for risk factors that lead to reductions in birthweight. Common prenatal exposures associated with a risk of reduced birthweight in full-term newborns include use of tobacco, alcohol, or other drugs.
| Recommendations for the General Populationa | C-8 Medical Panel Recommendationb,c for Class Members |
|---|---|
| Lower birthweight | |
| Screen for risk factors for low birthweight in pregnant persons during prenatal well visitd | No screening recommended for C-8 class memberse |
| Dyslipidemia (in adults and children) | |
| Screen all children once between ages 9 and 11 years and again between ages 17 and 21; among those with a familial history, begin screening at age 2 years and follow up yearlyf | Screen children for cholesterol levels at age 2 years and older unless already screened during the prior 5 years, already diagnosed, or receiving treatment |
| Screen adults aged 40–75 with no history of cardiovascular disease (CVD), one or more CVD risk factors, and a calculated 10-year CVD event risk of 10% or greaterg | |
| American Heart Association recommends all adults aged 20 or older have their cholesterol and other traditional risk factors checked every 4–6 years as long as their risk remains lowh | |
| Kidney cancer (in adults) | |
| No routine screening recommended | Screen individuals aged 20–39 years with a symptom questionnaire; follow up with abdominal exam and urine test if symptoms present Screen individuals aged 40 or older with a symptom questionnaire, abdominal exam, and urine testing |
| Decreased antibody response (in adults and children) | |
| No routine screening recommended | No screening recommended for C-8 class memberse |
| Breast cancer in adults | |
| U.S. Preventive Services Task Force (USPSTF): Screen average-risk women aged 50–74 with mammography every 2 yearsi | No screening recommended for C-8 class memberse |
| Women’s Preventive Services Initiative (WPSI): Screen average-risk women with mammography; mammography should be initiated no earlier than age 40 and no later than age 50 and occur annually or biennially until age 74 j | |
| Pregnancy-induced hypertension (gestational hypertension and preeclampsia) | |
| Screen pregnant persons for hypertension and preeclampsia throughout pregnancyk,l | Screen pregnant persons for hypertension and proteinuria throughout pregnancy |
| Liver enzyme alterations in children and adults | |
| No routine screening recommended | No screening recommended for C-8 class memberse |
| Testicular cancer in adults | |
| American Academy of Family Physicians (AAFP) and USPSTF recommend against screening asymptomatic adolescents and adults for testicular cancerm | Screen for testicular cancer with a physical exam and questionnaire |
| Thyroid dysfunction in adults | |
| Screen newborns as part of recommended uniform screening paneln | Screen adults’ serum thyroid-stimulating hormone; otherwise test based on signs and symptoms of thyroid dysfunction |
| No routine screening recommendedo | |
| Ulcerative colitis in adults | |
| No routine screening recommended | Screen for symptoms with questionnaire starting at age 15 years |
a In cases in which conflicting or differing recommendations for population-level screenings have been issued, the clinical practice guideline developers have been identified for clarity.
c The C-8 Medical Panel recommended that members of the class action lawsuit, Jack W. Leach et al. v. E.I. du Pont de Nemours & Company (no. 01-C-608 W.Va., Wood County Circuit Court, filed April 10, 2002), be screened once in 2013; the panel has since updated its guidance, and now recommends that class members be screened three times, 3 years apart (C-8 Medical Panel, 2022). See Chapter 1 for more details about the lawsuit.
e The C-8 Medical Panel was allowed to develop recommendations only for the six conditions identified by the C-8 Science Panel in 2013: pregnancy-induced hypertension, kidney cancer, testicular cancer, thyroid disease, ulcerative colitis, and hypercholesterolemia. The C-8 Medical Panel did not deliberate about screenings for lower birthweight, decreased antibody response, breast cancer, or liver enzyme functions (C-8 Medical Panel, 2013).
Kidney Cancer in Adults
There are no effective screening approaches for identifying kidney cancer early in its course, and therefore no authoritative clinical screening recommendations. Urinalysis is effective at finding blood in the urine, which can be a sign of advanced kidney cancer but is also indicative of other disorders, such as infections and kidney stones. The C-8 Medical Panel recommends that clinicians ask about family history, symptoms of kidney cancer (gross hematuria, chronic abdominal pain, recent involuntary weight loss, unexplained fever for 1 week), conduct a physical exam for abdominal mass, and check a urine dipstick for blood (C-8 Medical Panel 2013, 2022). Although palpation for an abdominal mass is not harmful, it is unlikely to lead to early detection and may provide false reassurance.
Decreased Antibody Response in Children and Adults
The predictive value of antibody titers after vaccination or infection is usually unclear, and the evidence for an association between PFAS exposure and infection risk or severity is insufficient. Nor are there any evidence-based recommendations or other clinical guidance for addressing decreased antibody response. This is an important area for additional research.
Outcomes with Limited Suggestive Evidence of Association
Breast Cancer in Adults
The USPSTF recommends biennial mammographic screening for all average-risk women aged 50–74 (USPSTF, 2016a). For women aged 40–49, the USPSTF states that the decision to start screening mammography should be an individual one, and that women who place a higher value on the potential benefit than on the potential harms may choose to begin biennial screening. For women aged 75 and older, the USPSTF makes no recommendation because of insufficient evidence (USPSTF, 2016a). The HRSA-supported Women’s Preventive Services Initiative recommends that average-risk women initiate “mammography screening no earlier than age 40 and no later than age 50,” that “screening mammography should occur at least biennially and as frequently as annually,” and that it “should continue through at least age 74 and age alone should not be the basis to discontinue screening” (WPSI, 2019).
Pregnancy-Induced Hypertension
Pregnancy-induced hypertension, including gestational hypertension and preeclampsia, affects about 1 in every 12–17 pregnant persons aged 20–44 in the United States, and poses serious health risks for pregnant persons and fetuses during pregnancy (Bateman et al., 2012). As part of standard prenatal care, pregnant persons seeing a clinician will have their blood pressure monitored routinely throughout their pregnancy to reduce various risks to both parent and fetus associated with high blood pressure (Kilpatrick, 2017). This standard measurement is feasible, and its benefits outweigh its harms. The C-8 Medical Panel reinforces the standard blood pressure monitoring recommendations (C-8 Medical Panel 2013, 2022).
Elevated Liver Enzymes in Children and Adults
Elevated liver enzymes do not represent a health outcome by themselves, although they generally indicate a level of liver inflammation. Elevations are often found incidentally with multiphasic blood test panels administered as part of routine medical care or as part of an assessment of patient symptoms or concerns. Elevated liver enzymes have many causes, the most common of which include use of over-the-counter pain medications (particularly acetaminophen) and certain prescription medications (including statin drugs), alcohol consumption, heart failure, viral hepatitis, fatty liver disease, and obesity. There are no authoritative recommendations for screening for liver enzyme alterations in otherwise healthy patients who are not being monitored for liver dysfunction, and follow-up recommendations for elevations depend on which enzymes are affected, the degree of elevation, and characteristics of the individual patient.
Testicular Cancer in Adults
Testicular cancer, though rare, is the most common cancer in American males aged 15–25 (NCI, n.d.). Most cases of testicular cancer are discovered incidentally by patients or their partners. The USPSTF found that there is inadequate evidence that screening by clinician examination or patient self-examination has a higher yield or greater accuracy for detecting testicular cancer at earlier stages. It is also not known whether earlier detection would lead to better health outcomes. The USPSTF concludes that there is no benefit of screening for testicular cancer in the general population and recommends against it (USPSTF, 2011). The C-8 Medical Panel recommends a risk questionnaire and clinical testicular exam, considering ultrasound if additional risk factors are identified (C-8 Medical Panel, 2013, 2022).
Thyroid Disease and Dysfunction in Adults
There are well-defined approaches for identifying and treating thyroid hormone dysfunction, especially among older adults and women (CDC, 2014). The standard clinical practice for identifying thyroid dysfunction is to order blood testing for levels of thyroid-stimulating hormone (TSH) when there are signs or symptoms that could be attributable to hypo- or hyperthyroidism (NIDDK, 2017). Standard approaches exist for diagnosis and treatment of thyroid disorders. In its review, however, the USPSTF concluded that the current evidence is insufficient to assess the balance of benefits and harms of screening for thyroid dysfunction in nonpregnant, asymptomatic adults. The C-8 Medical Panel recommends that adults in PFAS-contaminated communities receive TSH-level screening in addition to testing based on signs and symptoms (C-8 Medical Panel 2013, 2022).
Ulcerative Colitis in Adults
Ulcerative colitis is a chronic bowel disease with a prevalence of 1.3 percent among U.S. adults that results in inflammation and sores in the lining of the large intestine (colon) and rectum (Dahlhamer et
al., 2016). It can be debilitating and lead to life-threatening complications. In addition to such generalized symptoms as fatigue, fever, and weight loss, affected individuals experience abdominal pain; blood or pus in stool; rectal bleeding; and frequent, recurring diarrhea. Diagnosis requires endoscopy and laboratory testing (Hanauer, 2004). There are no authoritative recommendations for screening for ulcerative colitis. The C-8 Medical Panel recommends that clinicians administer a questionnaire to elicit symptoms of the condition beginning at age 15 (C-8 Medical Panel, 2013, 2022); however, no information is available regarding the accuracy of the questionnaire.
RECOMMENDATIONS FOR PATIENT FOLLOW-UP
Where appropriate, the committee developed recommendations for patient follow-up for PFAS-associated health outcomes that should be offered to patients based on shared, informed decision making between patient and clinician. The clinical practice guidelines for standard medical care and the C-8 Medical Panel recommendations served as the basis of these recommendations. Some conditions associated with PFAS exposure have no established clinical prevention guidance, while other clinical prevention recommendations are beneficial when applied in cases of increased risk. There is value in specifying follow-up that is part of the standard of care as defined by authoritative clinical professional groups because clinicians often are unable to deliver all recommended preventive services during primary care visits (Privett and Guerrier, 2021) and must decide with patients which services to focus on considering both evidence and patient values and preferences (USPSTF et al., 2022).
The committee used its three established cutoff levels for PFAS in serum or plasma (detailed in Chapter 5) to determine follow-up based on PFAS exposure level, although the risks are not the same within each of these three categories. The risks from PFAS likely increase with increased exposure thus PFAS levels of 3 nanograms per milliliter (ng/mL) and 19 ng/mL do not represent the same risk. PFAS blood testing measures burden at the time of sample collection. For example, a person with low blood levels today may have had higher levels in the past. Clinicians should use judgment and shared decision making in making follow-up decisions based on PFAS exposure and other risk factors. Figure 6-1 suggests that clinicians engage in shared, informed decision making with their patients regarding followup care for PFAS-associated health outcomes.
Recommendation 6-1: Clinicians should treat patients with serum PFAS concentration below 2 nanograms per milliliter (ng/mL) with the usual standard of care.
Recommendation 6-2: For patients with serum PFAS concentration of 2 nanograms per milliliter (2 ng/mL) or higher and less than 20 ng/mL, clinicians should encourage PFAS exposure reduction if a source of exposure is identified, especially for pregnant persons. Within the usual standard of care clinicians should:
- Prioritize screening for dyslipidemia with a lipid panel (once between 9 and 11 years of age, and once every 4 to 6 years over age 20) as recommended by the American Academy of Pediatrics (AAP) and the American Heart Association (AHA).
- Screen for hypertensive disorders of pregnancy at all prenatal visits per the American College of Obstetricians and Gynecologists (ACOG).
- Screen for breast cancer based on clinical practice guidelines based on age and other risk factors such as those recommended by the U.S. Preventive Services Task Force (USPSTF).
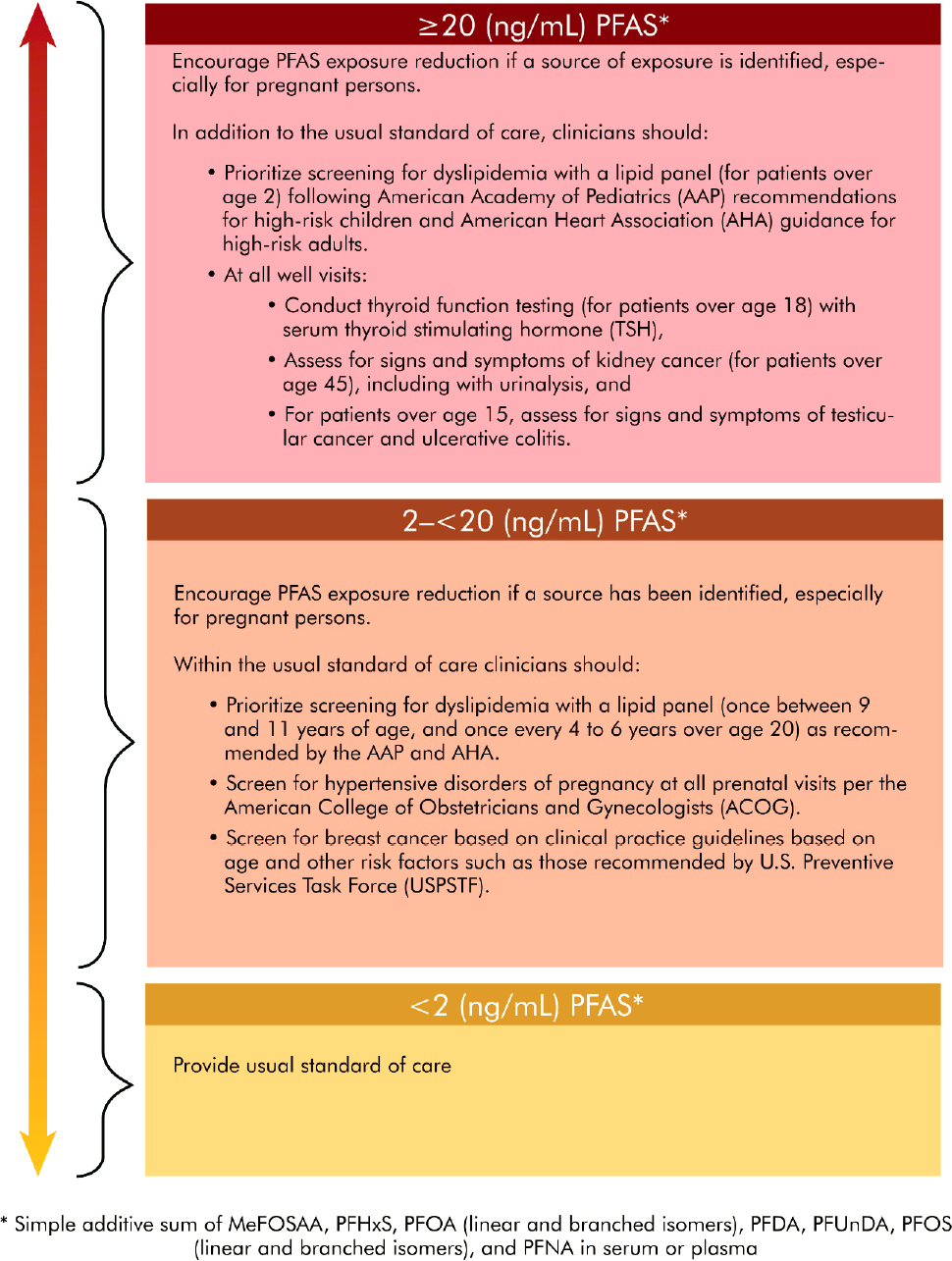
NOTE: MeFOSAA = methylperfluorooctane sulfonamidoacetic acid; PFDA = perfluorodecanoic acid; PFHxS = perfluorohexane sulfonic acid, PFNA = perfluorononanoic acid; PFOA = perfluorooctanoic acid; PFOS = perfluorooctanesulfonic acid; PFUnDA = perfluoroundecanoic acid.
Recommendation 6-3: For patients with serum PFAS concentration of 20 nanograms per milliliter (ng/mL) or higher, clinicians should encourage PFAS exposure reduction if a source of exposure is identified, especially for pregnant persons. In addition to the usual standard of care, clinicians should:
- Prioritize screening for dyslipidemia with a lipid panel (for patients over age 2) following American Academy of Pediatrics (AAP) guidelines for high-risk children and American Heart Association (AHA) guidance for high-risk adults.
-
At all well visits:
- conduct thyroid function testing (for patients over age 18) with serum thyroid stimulating hormone (TSH),
- assess for signs and symptoms of kidney cancer (for patients over 45), including with urinalysis, and
- for patients over 15, assess for signs and symptoms of testicular cancer and ulcerative colitis.
APPLYING THE COMMITTEE’S EXPOSURE, TESTING, AND CLINICAL FOLLOW-UP RECOMMENDATIONS
The Committee created a flow chart summarizing PFAS education, exposure assessment, and clinical follow-up (see Figure 6-2). In communities where PFAS exposure has been identified, the Agency of Toxic Substances and Disease Registry (ATSDR) and other government entities should support local clinicians with educational materials about PFAS exposure and testing. Clinicians should then determine whether a particular patient is likely to have a history of elevated exposure to PFAS. If so, the clinician should offer PFAS testing and make a shared, informed decision on that testing. If testing is chosen, the labs should be ordered (Test Code 39307, Current Procedural Terminology [CPT] Code 82542). Test results should be interpreted by summing the concentrations of MeFOSAA, PFHxS, PFOA (linear and branched isomers), PFDA, PFUnDA, PFOS (linear and branched isomers), and PFNA. The laboratory may not report results for all PFAS considered by the committee or may include different PFAS in their panel. In that case, the sum of PFAS should include only the PFAS in the analyte list considered by the committee. For example, if the lab tests for PFOA, PFOS, PFHxS, PFNA, and PFBS, the summation should include PFOA, PFOS, PFHxS, and PFNA. Differing analyte lists may cause some variation in test results. Still, as long as PFOA, PFOS, PFHxS, and PFNA are included in the analyte list, the results may not vary too greatly, as these four analytes are the ones most commonly detected in the United States. If any analyte is below the limit of detection, the clinician should calculate the analyte limit of detection divided by the square root of 2 and use this value in the summation. The summation should then be compared against Figure 6-2 to determine an appropriate clinical follow-up plan based on shared, informed decision making between patient and clinician.
CONCLUSION
The committee believes its clinical follow-up recommendations may be helpful to clinicians who have been asked to address PFAS-associated risks as part of routine health care delivery. There are potential harms both from aggressive clinical follow-up and from ignoring the risks of PFAS exposure. Clinicians and patients should decide which screening practices and services to pursue through a process of shared, informed decision making, along with consideration of the patients’ level of PFAS exposure and other risk factors they may have. For young children, these discussions will likely take place with the parents; for adolescents, shared, informed decision making is complicated and an active area of research (Boland et al., 2019). The committee’s patient follow-up recommendations should be updated as clinical practice guidelines change and as more is learned about the health effects of PFAS.
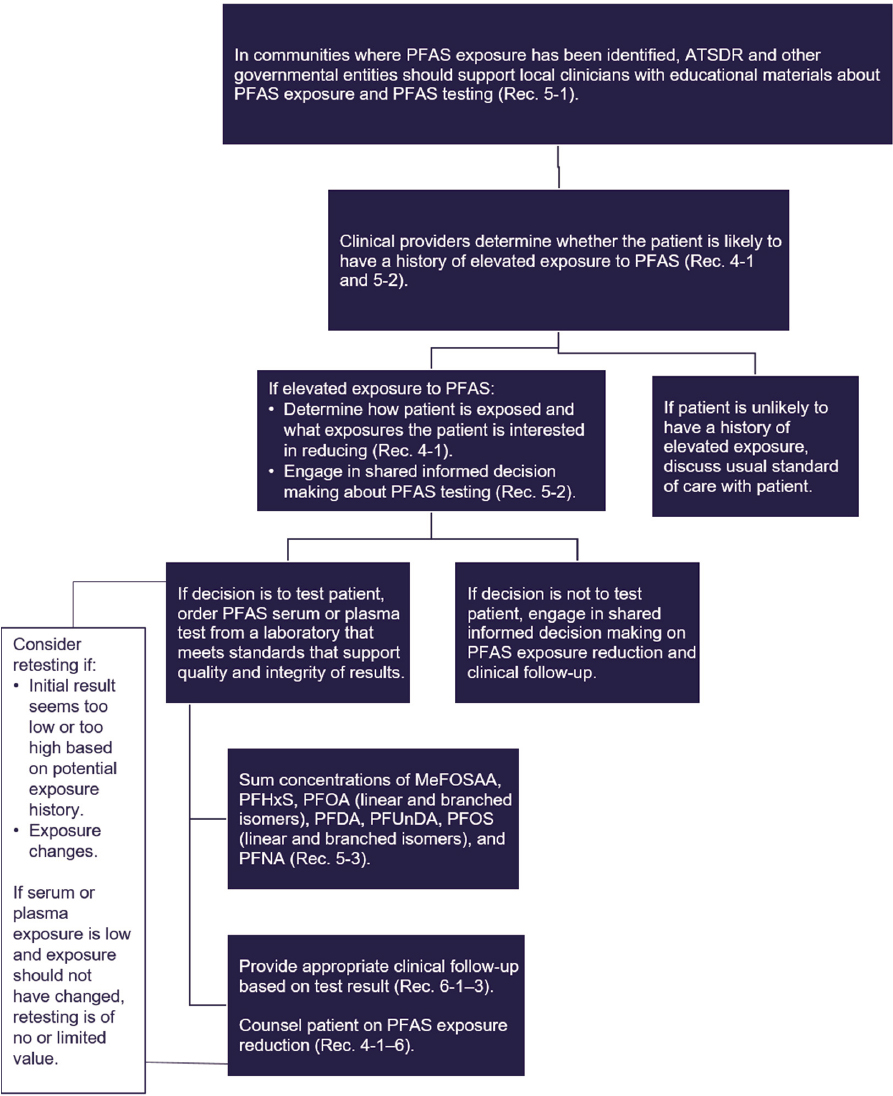
NOTE: ATSDR = Agency for Toxic Substances and Disease Registry; MeFOSAA = methylperfluorooctane sulfonamidoacetic acid; PFDA = perfluorodecanoic acid; PFHxS = perfluorohexane sulfonic acid, PFNA = perfluorononanoic acid; PFOA = perfluorooctanoic acid; PFOS = perfluorooctanesulfonic acid; PFUnDA = perfluoroundecanoic acid.
REFERENCES
AHRQ (Agency for Healthcare Research and Quality). 2020. The CAHPS ambulatory care improvement guide: Practical strategies for improving patient experience. https://www.ahrq.gov/cahps/quality-improvement/improvement-guide/improvement-guide.html (accessed July 1, 2022).
Bateman, B. T., K. M. Shaw, E. V. Kuklina, W. M. Callaghan, E. W. Seely, and S. Hernández-Díaz. 2012. Hypertension in women of reproductive age in the United States: NHANES 1999–2008. PLOS ONE 7(4):e36171. https://doi.org/10.1371/journal.pone.0036171.
Boland, L., I. D. Graham, F. Légaré, K. Lewis, J. Jull, A. Shephard, M. L. Lawson, A. Davis, A. Yameogo, and D. Stacey. 2019. Barriers and facilitators of pediatric shared decision-making: A systematic review. Implementation Science 14(1):7. https://doi.org/10.1186/s13012-018-0851-5.
C-8 Medical Panel. 2013. Information on the C-8 (PFOA) Medical Monitoring Program screening tests prepared by the medical panel for the C-8 class members. http://www.c-8medicalmonitoringprogram.com/docs/med_panel_education_doc.pdf (accessed January 28, 2022).
C-8 Medical Panel. 2022. C-8 Medical Monitoring Program. http://www.c8medicalmonitoringprogram.com (accessed January 28, 2022).
CDC (Centers for Disease Control and Prevention). 2014. HTDS Guide—About thyroid disease: Section summary. https://www.cdc.gov/nceh/radiation/hanford/htdsweb/guide/thyroid.htm (accessed January 28, 2022).
Dahlhamer, J. M., E. P. Zammitti, B. W. Ward, A. G. Wheaton, and J. B. Croft. 2016. Prevalence of inflammatory bowel disease among adults aged ≥18 years—United States, 2015. Morbidity and Mortality Weekly Report 65(42):1166–1169.
Grundy, S, M., N. J. Stone, A. L. Bailey, C. Beam, K. K. Birtcher, R. S. Blumenthal, L. T. Braun, S. de Ferranti, J. Faiella-Tommasino, D. E. Forman, R. Goldberg, P. A. Heidenreich, M. A. Hlatky, D. W. Jones, D. Lloyd-Jones, N. Lopez-Pajares, C. E. Ndumele, C. E. Orringer, C. A. Peralta, J. J. Saseen, S. C. Smith, L. Sperling, S. S. Virani, and J. Yeboah. 2019. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 139(25):e1082–e1143. https://doi.org/10.1161/CIR.0000000000000625.
Hagan, J. F., J. S. Shaw, and P. M. Duncan (Eds.). 2017. Bright Futures guidelines for health supervision of infants, children, and adolescents: Adolescence visits: 11 through 21 years. https://brightfutures.aap.org/Bright%20Futures%20Documents/BF4_InfancyVisits.pdf (accessed February 9, 2022).
Hanauer, S. B. 2004. Update on the etiology, pathogenesis and diagnosis of ulcerative colitis. Nature Clinical Practice Gastroenterology & Hepatology 1(1):26–31.
HRSA (Health Resources and Services Administration). 2018. Recommended uniform screening panel. https://www.hrsa.gov/advisory-committees/heritable-disorders/rusp/index.html (accessed January 28, 2022).
Kilpatrick, S. J., L-A. Papile, and G. A. Macones (Eds.). 2017. Guidelines for perinatal care (8th ed.). Elk Grove Village, IL: American Academy of Pediatrics.
NCI (National Cancer Institute). n.d. Cancer stat facts: Testicular cancer. https://seer.cancer.gov/statfacts/html/testis.html (accessed January 28, 2022).
NIDDK (National Institute of Diabetes and Digestive and Kidney Diseases). 2017. Thyroid tests. https://www.niddk.nih.gov/health-information/diagnostic-tests/thyroid (accessed June 30, 2022).
Privett, N., and S. Guerrier. 2021. Estimation of the time needed to deliver the 2020 USPSTF preventive care recommendations in primary care. American Journal of Public Health 111:145–149. https://doi.org/10.2105/AJPH.2020.305967.
Richerson, J. E., G. R. Simon, J. J. Abularrage, A. D. Arauz Boudreau, C. N. Baker, G. A. Barden, O. Brown, J. M. Hackell, and A. P. Hardin. 2017. Bright Futures guidelines. Pediatrics 139(4)85–87.
Schrager, S. 2018. Five ways to communicate risks so that patients understand. Family Practice Management 25(6):18–31.
USPSTF (U.S. Preventive Services Task Force). 2011. Testicular cancer: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/testicular-cancer-screening (accessed January 28, 2022).
USPSTF. 2015. Thyroid dysfunction: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/thyroid-dysfunction-screening (accessed January 28, 2022).
USPSTF. 2016a. Breast cancer: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-screening (accessed February 9, 2022).
USPSTF. 2016b. Statin use for the primary prevention of cardiovascular disease in adults: Preventive medication. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/statin-use-in-adults-preventive-medication (accessed February 9, 2022).
USPSTF. 2017. Preeclampsia: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/preeclampsia-screening (accessed January 28, 2022).
USPSTF. 2021. Hypertension in adults: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hypertension-in-adults-screening (accessed January 28, 2022).
USPSTF. 2022. Collaboration and shared decision-making between patients and clinicians in preventive health care decisions and U.S. Preventive Services Task Force recommendations. JAMA 327(12):1171–1176. http://doi.org/10.1001/jama.2022.3267.
Wilson, J. M., and Y. G. Jungner. 1968. [Principles and practice of mass screening for disease]. Boletín de la Oficina Sanitaria Panamericana 65(4):281–393.
WPSI (Women’s Preventive Services Initiative). 2019. Women’s preventive services guidelines. https://www.hrsa.gov/womens-guidelines-2019 (accessed February 9, 2022).












