
HIV and AIDS:
Global Collaboration to Combat a Mysterious Pandemic

The HIV and AIDS epidemic in the United States is often cited as a failure to take an epidemic striking a marginalized group seriously enough early in its emergence, a clear case for the power of citizens to move science forward, and ultimately a public health triumph. HIV and AIDS shaped how the United States considers, researches, and reacts to infectious disease, and the lessons of the epidemic need to be revisited and remembered in considering the future of public health in the United States and globally.
1981
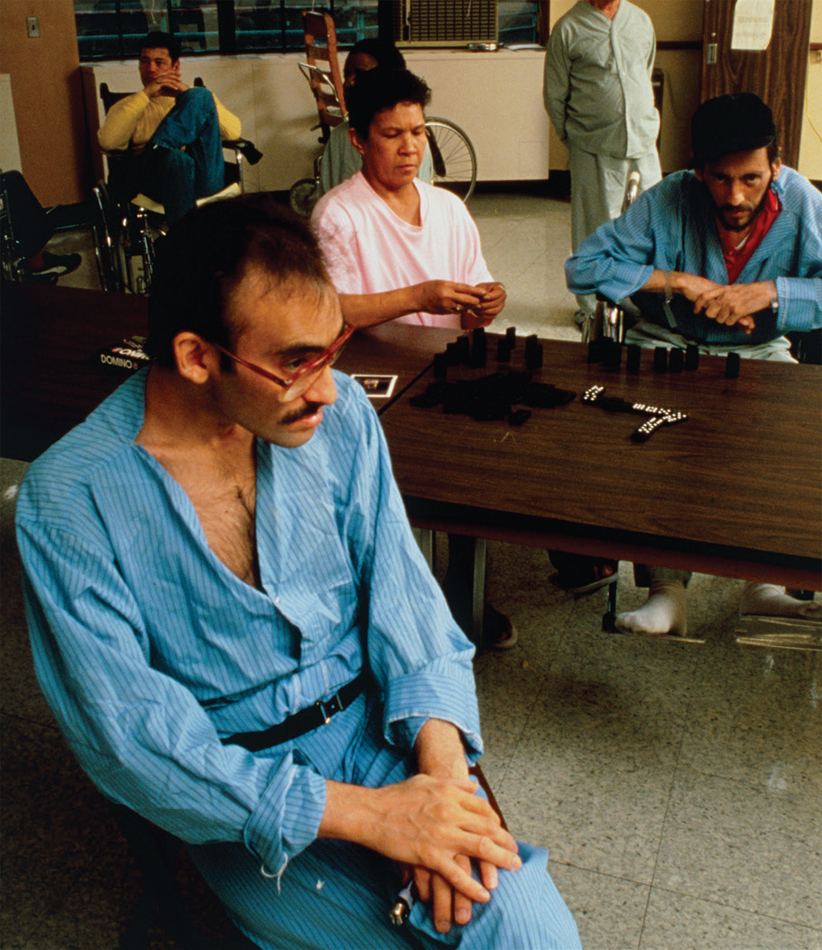
An Emergent Epidemic
On June 5, 1981, an article in the U.S. Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report identified rare, unusual infections in a cluster of young, White, gay men in Los Angeles. On the same day, a dermatologist reported an outbreak of Kaposi’s sarcoma, a rare skin cancer, among a small group of gay men in New York and California. This reporting, although not recognized as such until later, was the first official documentation of the acquired immunodeficiency syndrome (AIDS) epidemic.
1982
Settling on a Name
Because AIDS was initially identified and publicized in gay communities suffering from severe discrimination, the disease was highly stigmatized at first. The disease was initially called “Gay Men’s Pneumonia” in July 1980, which transitioned to the public shorthand “gay cancer” by the end of 1980. The New York Times called the disease GRID, or Gay-Related Immune Deficiency, in May 1982, and other media outlets referred to it as a “mysterious fever.” The Centers for Disease Control and Prevention adopted the use of the term AIDS, a comparatively neutral name, in September 1982, but the stigma associated with the disease persisted well beyond this date.


1983
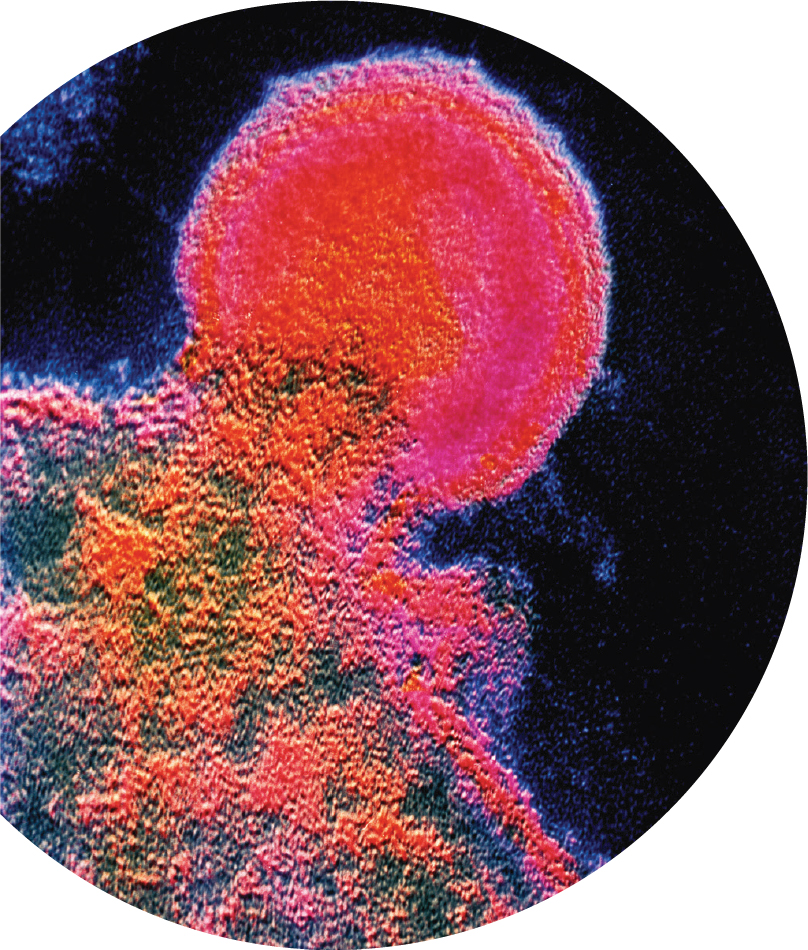
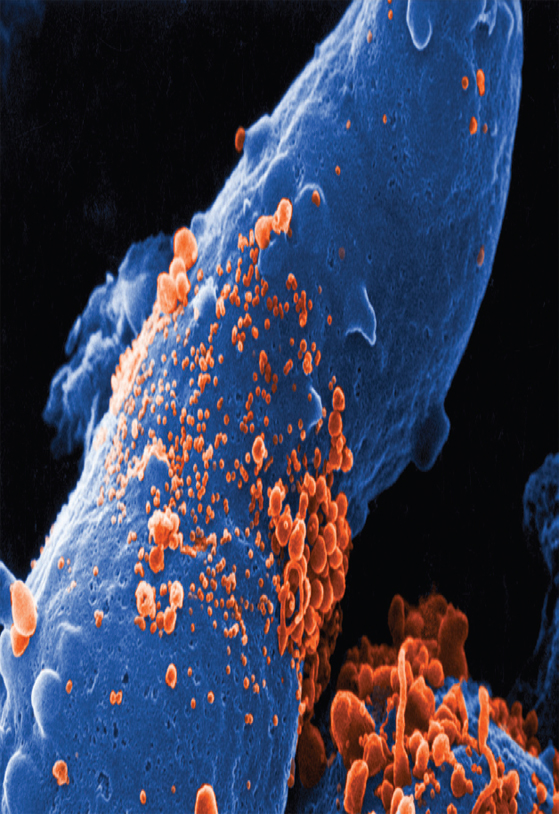
Identifying the Virus
In 1983, scientists at Institut Pasteur in France identified a retrovirus, or virus composed of RNA, that seemed to be attacking their patients’ immune systems and hypothesized that this retrovirus could be the cause of AIDS. The discovery of human immunodeficiency virus (HIV) was recognized by the 2008 Nobel Prize in Physiology or Medicine. Although transmission of HIV was first widely identified in men who have sex with men and in intravenous drug users, other vulnerable populations were quickly identified, including recipients of blood products, women who have sex with HIV-positive men, and children of HIV-positive pregnant women.
1986
Mobilizing a Response
Scientific, medical, and nonprofit organizations across the United States began to mount significant programs to combat the AIDS epidemic. In 1986, the Institute of Medicine and the National Academy of Sciences issued Confronting AIDS: Directions for Public Health, Health Care, and Research, making specific recommendations for a substantially increased effort to combat the spread of AIDS, through a $2 billion multifaceted program, including public health and media campaigns.

1987
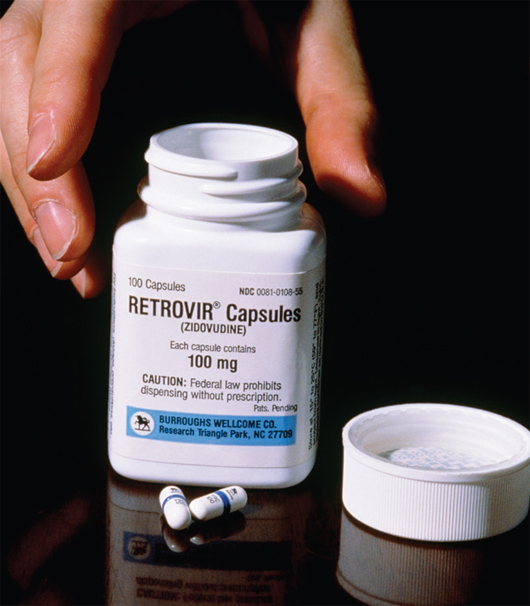
Expanding Access: Treatments and Regulations
In 1987, the first medication for AIDS was approved by the U.S. Food and Drug Administration (FDA)—azidothymidine, or AZT. This was not a new drug; rather, it had been developed to fight cancer, was found to be ineffective, and was shelved. Due to mounting public pressure and the increasing mortality burden of the disease, the FDA fast-tracked clinical trials of AZT—completing them in just 20 months, a speed unheard of previously. The FDA also provided expanded access to other experimental biologics during this time.
1989
Federal Support
As AIDS received more public attention in the latter part of the 1980s, the U.S. government, other governments, and international organizations began to provide dedicated funding and support to AIDS prevention, treatment, and education. The Health Omnibus Programs Extension Act was signed into law in 1988, which established the Office of AIDS Research at the National Institutes of Health and was the first federal bill in support of AIDS research and prevention. Congress also created the National Commission on AIDS in 1989, and the Ryan White Comprehensive AIDS Resources Emergency Act passed that same year, which allocated $221 million for care and treatment.
1996
Nearly Two Decades Later, Some Victories, and Significant Setbacks
Fifteen years after the AIDS epidemic was first identified, 1996 marked the first year in which new diagnosed cases declined. The next year the Centers for Disease Control and Prevention reported the first decline in AIDS-related deaths since 1981, attributed to newly approved and aggressive antiretroviral therapies. However, while AIDS appeared to be responding to controls in some communities, infections and deaths were increasing dramatically in Black and Latino(a)/Latinx/Hispanic communities. HIV infections were also growing at an exponential rate in Africa, and in 2000 the G8 released a statement calling for additional HIV/AIDS resources on a global scale. By 2020, more than 75 million people had been infected with HIV, causing more than 32 million deaths worldwide.

2003
Coordinating Efforts to Control the HIV/AIDS Epidemic
In 2003, the U.S. government created the Office of the U.S. Global AIDS Coordinator and Health Diplomacy to lead, manage, and oversee the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), the largest commitment ever made by a nation to address a single disease. Through PEPFAR, the U.S. government has invested over $90 billion in the treatment and prevention of HIV/AIDS around the world, saving more than 18 million lives and preventing millions of new HIV infections. PEPFAR’s emphasis on partnerships, sustainability, and data has guided the implementation of evidence-based interventions in the areas and populations with the greatest HIV/AIDS burden.
2011
Treatments Offer Hope
In 2011, two studies separately seemed to confirm that a daily dose of antiretroviral drugs can reduce transmission of HIV from an infected party to an uninfected party during sexual activity. Studies continued on the efficacy of pre-exposure prophylaxis, or PrEP, and in 2012 the U.S. Food and Drug Administration approved the first drug that can be taken daily to help prevent acquisition of the HIV virus through sexual activity. In 2015, the World Health Organization issued recommendations calling for all people living with HIV to begin antiretroviral therapy as soon as possible and recommended daily oral PrEP for all those who are at higher risk for contracting HIV. Despite these recommendations, many low-income and minority people remained at high risk for contracting HIV, did not have access to PrEP, and were contracting HIV at a higher rate than their White and wealthy peers.
That AIDS is no longer a certain death sentence remains one of the greatest public health success stories of recent decades. However, racial disparities that arose during the AIDS epidemic continue to exist today. Significant work needs to be done to ensure that low-income, racial minority, and transgender individuals who are at higher risk of HIV infection have the same access to PrEP that their wealthier White peers do. AIDS also continues to impact populations around the world, particularly in Africa, and the epidemic will not be over until it is contained globally.




