
Health Care Workforce Evolution:
Expanding and Diversifying the Health Care Team
The health care workforce changed dramatically in the five decades after 1970. New specialty roles emerged, such as hospitalists, intensivists, and emergency medicine, that altered the practice of medicine. Primary care models shifted from individual solo practice toward group practices and hospital-owned practices. New modes of payment changed how the workforce is compensated. Current and future needs, such as the aging of the population, are likely to lead to continued changes in the health care workforce.

1970s
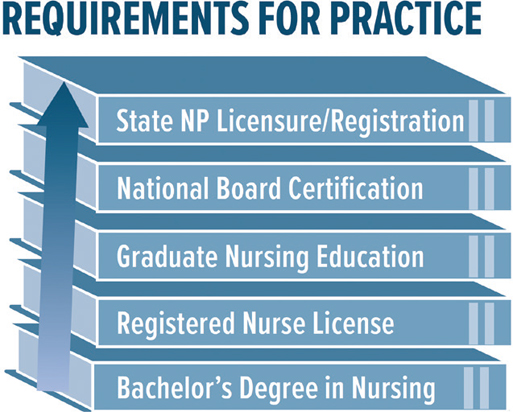
Advanced Nurse Practitioner Rules and Requirements
In the 1970s, policymakers concluded that, to provide all Americans with access to health care, the range of functions that nurses could perform should be widened. One result was new emphasis on an advanced nurse practitioner role that provided more autonomy and authority to nurses with advanced training. Though controversy initially surrounded the standards and regulations associated with advanced nurse practitioners, pivotal court cases—including a 1986 decision by the Texas Supreme Court—cemented their role in the health care professions.
1971
Physician Assistants Receive Recognition
After Duke University created the first education program for physician assistants (PAs) in 1965 as health insurance coverage expanded, a physician shortage intensified, and the need for better access to health care grew in underserved areas of the United States. Such programs trained people with previous medical experience, often returning military corpsmen, to become generalist assistants who could help physicians with a variety of tasks. In 1971, the American Medical Association recognized the PA profession and began work on national certification procedures. As PAs received more recognition for their contributions to the medical workforce, the 1986 Omnibus Budget Reconciliation Act expanded Medicare coverage of their services, positioning the profession for a period of rapid growth.


1978
Elevating Primary Care
Primary care is a critical source of health care in the United States, but the term was poorly defined historically, resulting in inconsistent care. The Institute of Medicine first defined primary care in 1978 and then refined the definition in 1996 as “the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community.” By addressing the roles of the patient, family, community, and delivery system, this definition has made it easier for primary care to be provided in a standard way. In 2021, the National Academies of Sciences, Engineering, and Medicine released Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care, which puts forth an evidence-based plan to strengthen primary care services in the United States, especially for underserved populations, and to inform primary care systems around the world.

2000s
Expanding the Ability to Prescribe Medications
As record numbers of physician assistants (PAs) entered the workforce in the early 2000s, and as physician assistant education programs expanded and improved, policymakers began to reconsider the breadth of services that PAs were able to provide. More and more states started allowing PAs to prescribe medications, though laws regarding controlled medications differed among states. Since 2007, when Indiana passed legislation providing prescriptive authority to PAs, all 50 states, the District of Columbia, and Guam have allowed PAs to prescribe medications.

2010
The Patient Protection and Affordable Care Act and the Health Care Workforce
Passage of the 2010 Patient Protection and Affordable Care Act expanded health coverage for millions of individuals while simultaneously increasing primary care capacity. The legislation provided incentives for medical school students and practicing physicians to enter primary care. It also encouraged more use of nurse practitioners and physician assistants in providing such care.

2010
Changes to the Nursing Profession
In 2010, the Institute of Medicine (IOM) recommended that to manage increasingly complicated patient conditions, at least 80 percent of registered nurses should hold a bachelor’s degree by 2020, and this call was echoed by the American Association of Colleges of Nursing (AACN). In response to these recommendations, the capacity of 4-year nursing programs has greatly increased, and enrollment has risen rapidly in nursing baccalaureate degree programs. The IOM and the AACN also urged nurses to continue their education into graduate and postgraduate programs to fill the nation’s demand for advanced practice registered nurses, who can offer many of the same services as physicians. Today, nurses have a much broader scope of duties than they once did: providing patient care, serving as patient advocates, leading health care teams, and conducting research to improve care.
2017
Identifying Medical Assistants
Until the 1950s, assistants who helped physicians carry out their work lacked a formal title or organization. In the second half of the 20th century, these attendants became known as medical assistants (MAs), though their responsibilities evolved over time. By 2017, California had defined medical assistants as unlicensed individuals who perform basic administrative, clerical, and technical supportive services under the direct oversight of a supervising physician or a physician-delegated supervisor. MAs may not diagnose, treat, or perform any task that is invasive or requires an assessment, and the physician is ultimately responsible for any services provided by an MA.

2018
Empowering Nurses
Nursing Now launched in 2018 as a 3-year global campaign to improve health by raising the profile and status of nursing worldwide. Run in collaboration with the World Health Organization and the International Council of Nurses, Nursing Now seeks to empower nurses to take their place at the heart of tackling 21st-century health challenges and to maximize their contribution to achieving universal health coverage. The campaign sought to ensure that nurses and midwives have a more prominent voice in health policymaking, encourage greater investment in the nursing workforce, recruit more nurses into leadership positions, conduct research that helps determine where nurses can have the greatest impact, and share best practices in nursing.

Technological innovations, the shift to value-based care, increased regulations and reporting requirements, and rapidly changing consumer expectations will require both a larger health care workforce and a more holistic view of health care delivery. Technology can increase health care capacity, reduce administrative burden, and augment human capabilities, but these innovations place demands on already stressed health care professionals. Making the most of future advances will require the rapid incorporation of new roles and new skills into delivery models.




