
Medical and Health Informatics:
Applying Digital Technology to Transform Care, Health, and Learning

As computers became smaller and more portable in the 1970s, they became increasingly effective tools in hospitals and clinics. Building on early experiences with digital patient scheduling and order entry systems, the clinical record began to undergo digitization. Nevertheless, the vast majority of health care providers continued to use paper charts throughout the 20th century.

1970
Pioneering the Field of Medical Informatics
In 1970, the new Division of Clinical Computing at Beth Israel Deaconess Medical Center, extending work done previously in universities and health systems, began seeking to improve the delivery of health care by harnessing information technology. The division’s visionary leaders predicted early on that paper charts would become extinct and advocated for digital medical records.
1970s
Putting Technology into Practice
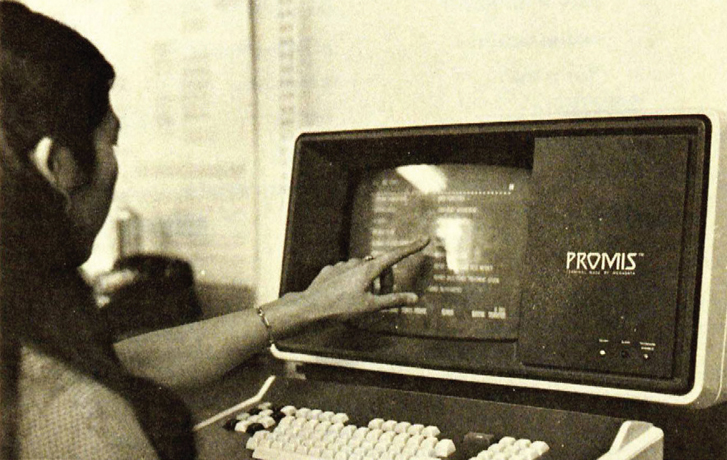
In the 1970s, physicians began to work more closely with computer scientists to expand the capabilities of the electronic health record. The Computer Stored Ambulatory Records system at Massachusetts General Hospital, The Medical Record at Duke University, the Problem-Oriented Medical Information System (PROMIS) at the University of Vermont, Health Evaluation through Logical Programming, and the Technicon Medical Information System were among the first systems that could store patients’ data and provide information for patient management and research.
1987
Setting Standards and Regulating Health Information Technology
The nonprofit standards-developing organization Health Level Seven International (HL7) was founded in 1987 to set standards for the sharing of electronic health information to support clinical practice and the delivery of health services. HL7 is notable for its expansion to include diverse members—including health care providers, government stakeholders, payers, pharmaceutical companies, vendors and suppliers, and consulting firms—to promote cross-sector collaboration. In 1990, the National Library of Medicine released the first edition of its Unified Medical Language System Knowledge Sources to promote interoperability between computer systems, and the 1996 Health Insurance Portability and Accountability Act established a process for establishing national standards. Standards-setting organizations are key to establishing baseline expectations and evaluating the processes of organizations that are expanding their use of health information technology.
1988
Building an Informatics Community
The American Medical Informatics Association (AMIA), which formed through the merger of several pre-existing scientific and engineering organizations, launched in 1988 to advanced the science of health informatics and to ensure that health information technology is used effectively to promote the provision of health care. AMIA connects professionals and students interested in informatics and serves as an authoritative voice in the field through the efforts of its members, who continue to drive thought leadership, research, and practice in their respective disciplines.
2000
Considering Patient Privacy in Health Information Standards
In 2000, the Standards for Privacy of Individually Identifiable Health Information (also known as the Privacy Rule) established, for the first time, a set of national requirements for the use and disclosure of individuals’ health information. The Privacy Rule applies to health plans and any health care provider who shares health information electronically in connection with the Health Insurance Portability and Accountability Act. The Privacy Rule communicates to patients how their health information is used and grants them more control, protecting their privacy rights and enabling the flow of information for high-quality health care.
2004
Pledging to Implement Data Exchange Standards
In 2004, the Office of the National Coordinator for Health Information Technology was created, a watershed moment for health information technology. This office produced the Nationwide Health Information Network, which provided a new set of standards for nationwide health information exchange. Participating organizations sign a legal agreement outlining their roles and responsibilities and agree to have the appropriate measures in place to protect the data shared among participants. The network provides a foundation of security, quality, efficiency, accountability, and governance that extends across varying federal, state, and local policies and laws.
2009
Getting Providers Across the Nation on the Same Page
Passage of the American Recovery and Reinvestment Act in 2009 required that 70 percent of primary care providers adopt electronic health records in the next 5 years. The act led to the funding of national, state, and regional informatics-related projects, including disease and health tracking, the establishment of research centers offering technical assistance, and the development of best practices in health information technology. The act marked a trend of growing recognition of the field of medical informatics and its potential to contribute to the health care arena while establishing the adoption of health information technology as a national priority.

2015
Interoperability to Improve Health
The publication of Connecting Health and Care for the Nation: A Shared Nationwide Interoperability Roadmap in 2015 by the Office of the National Coordinator for Health Information Technology laid out the near-term milestones and commitments expected of stakeholders to prioritize health information technology. The roadmap identified four pathways to pursue: improving technical standards and implementation guidance for priority data domains; rapidly aligning federal, state, and commercial payment policies from fee-for-service to value-based models; aligning federal and state privacy and security requirements that enable interoperability; and coordinating stakeholders to promote consistent policies and practices that support interoperability.

2020
Updating Requirements for the 21st Century
To increase efficiency and reduce administrative burden and costs, the Office of the National Coordinator for Health Information Technology released a new rule in 2020 on interoperability and information blocking—that is, any action likely to interfere with, prevent, or discourage access, exchange, or use of electronic health information. These regulatory changes created a more well-defined framework for health information technology vendors to improve the flow of data across disparate systems in support of big data analytics, population health management, and value-based care.

Since 1970, increasing recognition of the potential for digital technologies to aid in diagnoses, record keeping, information sharing, and care coordination has spurred efforts to institute electronic health records. Today, almost all hospitals in the United States have at least a basic electronic health record system, and many have more comprehensive systems that aid in diagnoses and enhance quality of care. However, issues of interoperability and privacy protections continue to hinder the integration of disparate systems. Advances in information technology—including speech recognition, artificial intelligence, predictive analytics and consumer-facing tools that can be integrated into health information systems—have begun to improve the quality, safety, and value of care, with much promise to further improve health and health care delivery.




